35 Strip Excision Techniques
Summary
Keywords: strip harvesting FUT transection rate minimizing trauma maximizing donor hair
Key Points
•A combination of superficial sharp incision followed by deep blunt dissection or dissection under visualization achieves the most consistently precise strip removal.
•The two most popular techniques to minimize hair transection in strip harvesting are the skin hook and spreader methods.
•It is vital to master more than one way to excise the donor strip to ensure quality grafts in a variety of circumstances.
35.1 Introduction
There have been many approaches to strip donor harvesting over the years. In the beginning, multibladed scalpels were used. When multiple sizes of micro- and mini-grafts were used and very little tissue was discarded, the transections that occurred had less significance, as the hairs would often grow in either the donor or the recipient site. However, with all follicular unit (FU) transplantation, it became clear that the multibladed scalpel in many cases caused an unacceptable amount of loss of follicles. The single-blade harvest was clearly superior. In skilled hands, the transection on the edges was routinely less than 5% and often even as low at 3%. The problem lay in the steep learning curve and difficult patient harvests—those with scar tissue, curly hair, and significantly changing hair directions. The skill of the surgeon in strip excision within this method of donor harvesting lies in keeping the scalpel blade parallel to the hair shafts to minimize follicle transection. Some form of blunt dissection may be particularly helpful in minimizing this transection rate and preserving the maximum number of follicles.1,2,3
Methods of Strip Harvesting
•Single-blade scalpel
•Double-blade scalpel
•Multiblade scalpel
•Hemostat technique
•Skin hook technique
•Spreader technique
Hair transplant procedures using the strip technique, harvesting 2,000 to 3,000 FU grafts (up to 7,000 hairs), are standard practice. In such cases, the donor strip can measure in the region of 30 cm in length, with over 500 grafts or 1,200 hair follicles along the upper and lower incision lines that are at risk of damage by transection. If all these are indeed transected, then the transection rate could be 17% and may be more if the surgeon lacks experience.4
The blind technique of harvesting with single- or multiple-bladed scalpels that cut all the way down to the bulbs in one stroke can often produce a high and unacceptable rate of transection.5 See Video 35.1a and Video 35.1b on strip harvesting pearls and tips.
35.2 Single-Blade Sharp Dissection Technique
Surgeons with extensive experience may still use this technique to harvest a strip. As mentioned previously, the danger of transection is greater, especially when used by surgeons with limited experience. This danger can be minimized when the blade is gently “dragged/pulled” along the incision, rather than using more force to push the scalpel. Checking the wound edge along the way, the surgeon can make small adjustments if transection is noted or they can convert to another harvest method. Tumescence can be especially helpful if it is injected at a consistent level along the length of the strip. If the level of infiltration is inconsistent, it can actually complicate the excision and increase the risk of transections. See Video 35.2 for demonstration of strip harvesting from start to finish.
35.3 Blunt and Direct Visualization Dissection Techniques
In 2003, Arturo Sandoval introduced a novel harvest technique, the “Sandoval Score and Spread,” which involved making a 1- to 2-mm superficial scoring incision, followed by a puncture of this incision with an arterial forceps (hemostat or mosquito), opening the forceps while inside the tissue applying sufficient force to separate along a natural plane of dissection, minimizing the potential transection from sharp dissection. The main disadvantage of this technique was its nonergonomic nature, making it painful to the fingers, as the weak finger muscles were used exclusively.6
Addressing the same issue and roughly around the same time, Damkerng Pathomvanich introduced the skin hook harvesting technique, which he called the “open technique.” This also involved a 1- to 2-mm scoring incision, but was followed by using skin hooks to apply outward traction on the wound edges. A scalpel blade was then used to gently tap the tissue under tension, and the follicles separated cleanly along the same plane of dissection.2,7,,,8,,9
Around 2005, Robert Haber introduced his tissue spreader that basically consists of a modified iconoclast instrument (Fig. 35.1a), onto which two sets of staggered prongs were attached (Fig. 35.1b). The prongs are used to separate the wound edges instead of the forceps or the hooks, with the advantage of using the more ergonomic strong hand muscles in a closing motion, as opposed to the weak finger muscles in an opening motion of the arterial forceps.4,6

The concept of the natural plane of tissue dissection is supported by histologic analysis of the FU, around which is a circumferential band of collagen oriented differently from collagen further from the FU. The junction of these two areas of collagen is likely this plane of separation.10
35.4 Skin Hook Direct Visualization Technique
This requires fairly simple instruments including single or double skin hooks, no. 15 or 10 surgical blades, and of course magnifying loupes. The technique should allow paramount clear visualization to achieve not only minimal follicle transection but also effective hemostasis. This usually requires sufficient tumescent fluid producing a nearly bloodless field.11,12
The initial incision is made superficially in what the author likes to call “deep scoring,” probably around 2 mm deep from the surface going just beyond the full epidermis, using a number 15 blade along the predetermined marker pen line, using the undersurface of the blade rather than the front tip. Standing slightly to the left of the patient in the sitting up position or slightly to the left of the incision line in the prone position, the author incises in a forward direction (reverse incision). This technique enables clearer visualization of the angle of the hairs especially if sufficient tumescent fluid is injected to make the hair exit angle less acute. This effect is further facilitated as the author lifts on the skin with his left thumb immediately ahead of the blade moving forward. The tumescent and pulling back on the skin have the added effect of firming the skin surface for better control of depth of incision. With the blade held with the right hand, the author further uses the right edge of the hand (resting down on the scalp) to stabilize the blade and further aid in control of the incision making. Skin hooks are then inserted into the exposed dermis on each side of the incision, and deeper more blunt dissection begins.1,2,11,,,12,,13
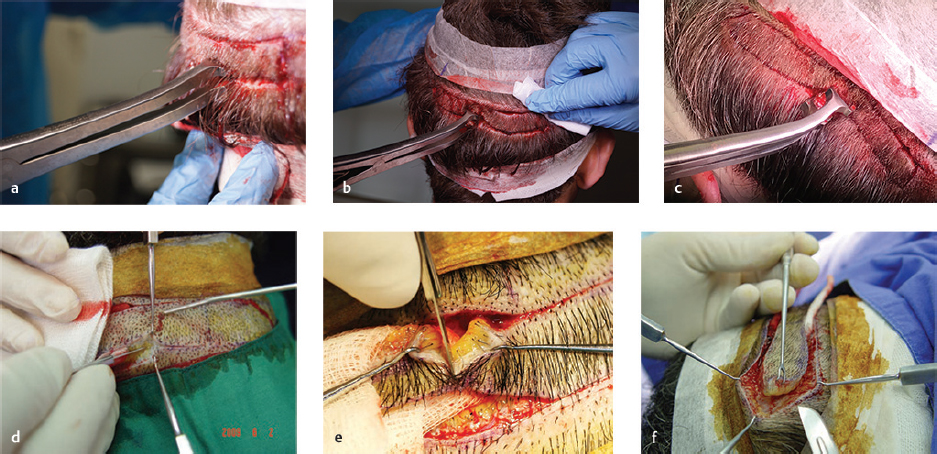
The skin hooks used can vary between two and four, depending on preference, tissue flexibility, number of surgical assistants available, and whether the harvesting is performed in the prone or sitting up position (Fig. 35.2a–c). The author prefers the sitting up position where the author holds one skin hook with his left hand pulling upward on the upper edge (or pulling to the left if the patient is prone), while his assistant pulls down on the lower wound edge (or to their left if the patient is prone with the assistant sitting across from the surgeon) holding another skin hook with their left hand.
Related posts:
 Methods and Techniques to Study Hair Cell Survival
Methods and Techniques to Study Hair Cell Survival
 Hair Transplantation: The Promise of Cell Therapy
Hair Transplantation: The Promise of Cell Therapy
 The Patient with Minimal Hair Loss: Planning and Decision-Making
The Patient with Minimal Hair Loss: Planning and Decision-Making
 The Young Patient: Planning and Decision-Making
The Young Patient: Planning and Decision-Making
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 East,West, and Southern Asian Hair Transplant Specifics
East,West, and Southern Asian Hair Transplant Specifics
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


