div class=”ChapterContextInformation”>
2. Intralesional Steroids: When and How to Inject?
Keywords
AlopeciaSteroidsIntralesionalTriamcinoloneBetamethasoneAtrophyHairAlopecia areataCicatricial alopeciasAcne keloidalisDiscoid lupusLichen planopilarisDissecting cellulitisFolliculitis decalvansAdrenal suppressionIntroduction
Intralesional steroid (IL-S) injections have been used to treat a variety of dermatological and nondermatological diseases. Infiltration of IL-S is a relatively simple, effective, and minimally invasive procedure. It allows transposition of the epidermal barrier, delivering the drug directly into the involved area. In addition, “targeted” treatment with IL-S prevents the occurrence of adverse effects related to the systemic use of the drug. In the treatment of alopecias, IL-S are an important therapeutic tool for many types of both scarring and nonscarring hair loss [1, 2]. For patchy alopecia areata in adults, for example, it is commonly considered as a first-line therapy [3]. This chapter will cover important topics for the daily practice of a physician in charge of patients with alopecia.
Which Intralesional Steroid Should I Use?
There are a few options of steroid salts available for intralesional use in dermatological conditions. The majority of studies report data from the use of triamcinolone acetonide (TA) which is widely used for the treatment of alopecias [2, 4]. However, other injectable steroids have also been studied, including triamcinolone hexacetonide (TH) [5], the associations of betamethasone dipropionate with betamethasone disodium phosphate [6], the acetate salt with betamethasone disodium phosphate [7], and dexamethasone acetate with dexamethasone disodium phosphate [8].
TH is known to be much less soluble than other steroids (including TA), increasing the risk of local side effects such as cutaneous atrophy [9]. Some authors have even considered TH to be unsuitable for intralesional injection due to its long half-life [1]. For this reason, using intralesional TH to treat cutaneous lesions should be regarded with caution.
One study from 1974 with healthy individuals investigated adverse events of intradermal injections of betamethasone acetate-phosphate 6 mg/mL suspension in comparison to triamcinolone 40 mg/mL preparations. Hypopigmentation, atrophy, and telangiectasia were much more marked and persistent at the sites of triamcinolone injection than in the areas injected with betamethasone. On the other hand, suppression of the pituitary-adrenal axis in individuals occurred with different doses of betamethasone, while injections of up to 20 mg of triamcinolone had no effect on cortisol levels [7].
Considering the more robust data on the use of TA and personal experience, this author has preference for TA in the treatment of patients with hair disorders.
Which Drug Concentration Should I Use?
Concentrations of TA used to treat patches of alopecia on the scalp commonly range from 5 to 10 mg/mL in most papers and textbooks [10, 11]. For patches involving the beard, eyebrows, or any other area outside of the scalp region, lower concentrations are generally recommended (up to 2.5 mg/mL of TA), although some authors have used the same concentrations in these sites (up to 10 mg/mL) as on the scalp [10, 12]. However, recent data has favored the use of lower concentrations of IL TA in alopecia areata patients. In a double-blind, placebo-controlled study, injection of 2.5 mg/mL of TA was as beneficial as 5 or 10 mg/mL for limited, patchy alopecia areata of the scalp. According to the authors, using the lowest effective concentration minimized the risk of local side effects of skin atrophy and telangiectasia and likely reduces the potential for systemic adrenal suppression. In addition, utilizing lower TA concentrations also allows for injection of a greater volume, increasing the maximal treatment area [13].

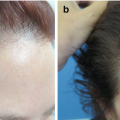
Frontal fibrosing alopecia: the skin between the old and new hairlines is atrophic

Acne keloidalis nuchae presenting with prominent fibrotic tissue
As a general rule, this author uses concentrations of up to 5 mg/mL of TA for the scalp and 2.5 mg/mL for the eyebrows and other facial areas. When atrophy is present, other treatments should be considered. If IL-S are used, lower concentrations are advised. When the atrophogenic effect is desired, as in cases above mentioned, 10 mg/mL of TA (or higher) can be used. The vascular patterns are better seen with the use of immersion fluids.
What Is the Best Way to Dilute Steroids for Intralesional Injections?
IL-S may be administered diluted in local anesthetics or isotonic saline solution. The diluent is generally a matter of personal choice, but some points need to be considered.
The acidic pH of lidocaine can cause an unpleasant burning sensation when the medication is injected. Intralesional injections of steroids are relatively fast procedures. The time interval between each skin puncture may not be enough for the onset of the anesthetic effect on the adjacent skin, and every puncture will end up being painful for the patient.
A particular situation refers to conditions with prominent fibrosis, such as acne keloidalis or folliculitis decalvans. In these cases, medication injected exerts great pression on the adjacent tissue, and patients may complain of pain for several minutes or even hours after the procedure. Using lidocaine as the diluent here will provide greater comfort after the injections.
An important point to consider is that the hexacetonide salt of triamcinolone should not be mixed with diluents or local anesthetics containing preservatives, such as parabens or phenols, since they may cause precipitation of the steroid increasing the risk of steroid deposition in the dermis and tissue atrophy [5, 14].
This author mainly uses isotonic saline solution as the diluent for IL-S injections. The exception are cases with prominent fibrosis, in which lidocaine is preferred.
The Technique
- 1.
First, the steroid should be diluted to the desired concentration.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree