Spine and pelvis issues in Major League Baseball do not often get the publicity that other, more common injuries do. However, despite low incidence rates involving significant time loss, there is a very high percentage of players who report having some lumbopelvic discomfort at some point in their careers. Baseball athlete’s bodies have unique clinical baseline presentations throughout the kinetic chain representing the unique demands of the game. The authors aim to outline a plan that can identify potential problematic presentations, implement an efficient and effective plan of care that will limit potential pain and injury, and maximize performance.
Key points
- •
This article focuses on lumbopelvic injury etiology and epidemiology.
- •
The authors discuss common injury prevalence and treatment.
- •
Lumbo-pelvic-hip dysfunction on baseball performance is also discussed in the article.
- •
Preventative measures including the following are discussed:
- ○
Consistent assessment.
- ○
Range of motion and strength normalization.
- ○
End range of motion strength and stability.
- ○
Video content accompanies this article at http://www.sportsmed.theclinics.com .
Introduction
Known as America’s pastime, baseball continues to be one of the most popular and participated across all sports. In 2022, over 2 million children played little league baseball with 400,000 moving onto high school baseball and 36,000 at the National Collegiate Athletic Association level. Opportunities to play also continue to grow with high school teams, travel baseball, private training, and showcases, which all provide the ability to improve necessary skills. Most of these players work hard and dream of the opportunity to be one of the 945 players on Opening Day rosters in Major League Baseball (MLB). This ample opportunity also provides compounding stress if not monitored correctly.
As a game, baseball is a combination of periods of inactivity followed by explosive movements, which incur some of the highest angular velocities and end ranges of motion seen in sports. The demands of the game are similar but can offer significant differences between the different positions. The most drastic difference is between pitchers and position players. However, regardless of position, all baseball players can be described as high-level rotational athletes working at the elite end of the biomechanical spectrum.
Due to the nature of the game, baseball players present with a unique clinical presentation. Baseline range of motion, mobility, and strength assessments are often outside of what would be considered normal in the general population. , Monitoring these presentations in the context of the specific population can contribute to a player’s ability to stay healthy and ultimately perform at a high level. Demands on MLB players outside of game play are also unique. An MLB season can be considered one of the most grueling schedules in sports. The season begins with a 7-week preseason camp including 30 games. This is followed by a 6-month season with an average of 6.3 games per week. Most months have 2 to 3 scheduled off days total. Combine this with cross-country, overnight travel, and the demands on the musculoskeletal system and the total allostatic load the body incurs are unlike any other sport.
Spine and pelvis injuries receive little attention compared to the more common shoulder and elbow injuries within baseball. However, a healthy and functional spine and pelvis are necessary for all required activity in baseball players. While spine and pelvis injuries have low occurrences and time loss statistics, over 85% of collegiate baseball players report having at least 1 bout of limiting low back pain in their careers. Given the violent nature of a baseball player’s swing or pitch, it is reasonable to believe that even the mildest change in alignment, mobility, or strength in the lumbopelvic region can have a direct impact on overall biomechanics and game success.
The authors hope to outline a reasonable, applicable plan for daily assessment and treatment to optimize player availability for game activity as well as positively influence performance.
Discussion
Baseball Player Game and Presentation Description
Historically, nontraumatic shoulder and elbow injuries have been associated with baseball players compared to other sports. The rise in elbow injury has led to increased media coverage as injury occurrence rises especially among a much younger patient population. Often overlooked, but just as important in the authors’ opinion, is the lumbo-pelvic region in baseball players regardless of position played.
Acute-onset spine and pelvis injuries have a low incidence rate of 1.8 per 1000 athlete exposures in college baseball players at practice and 5.8 per 1000 athlete exposures in game play. Most time loss is due to atraumatic, progressive impairment leading to dysfunction and pathology. These are most common during growth spurts and times of rapid increase in workload. , It has been noted that these overuse injuries tend to occur in the ramp up phase of the season lending to the focus on workload monitoring to allow for appropriate recovery from microtrauma and the lumbar spine and pelvis are no exception. Common diagnoses include muscle strains, spondylolysis, facet joint dysfunction, disk herniation, and sacroiliac-generated pain and it is not uncommon to find asymptomatic pathology on imaging studies. However, 75% to 89% of baseball players report having at least 1 bout of low back pain at some point in their careers. College baseball players have 3.23 times higher incidence of degenerative disk disease compared to the general population.
Since baseball is typically an asymmetric sport where repetitive loads are most often in 1 direction, maladaptation of tissues and pathology will follow suit. Moreover, microtrauma lends to articular nociceptive afferent activity which can cause abnormal posture and movement resulting in localized impairments. Altered clinical presentation of the lumbo-pelvic-hip complex described in the following paragraphs also cannot be ignored. Positional faults of the pelvis, altered orientation and mobility of the lumbar spine, and asymmetric hip mobility can lead to altered kinematics and tissue loading. This can lead to poor performance and possibly time lost due to pathology within the spine or other joints. , The atraumatic overuse nature of lumbopelvic injuries in baseball speaks to the impairment level contribution to pathogenesis of these injuries. Many of these pathologies can be seen on baseline examination in asymptomatic baseball players. This leads us to believe that with proper monitoring and programming, these athletes can restore and maintain lumbo-pelvic-hip function in order to remain healthy and successful.
Role of the spine and pelvis in baseball players
The unilateral and repetitive nature of maximum intent activity (throwing and hitting) involving higher ranges of motion compounded with increased frequency of competition creates a unique baseline presentation. As described by Gracovetsky in 1997, the kinetic chain is linked from lower to upper extremity through the cross-links surrounding the spine and pelvis. , Fascial sling connections such as the latissimus dorsi into the contralateral gluteus maximus provide a greater amount of stiffness during high-force and angular velocity movements such as hitting, throwing, and pitching and are integral in the combined motions needed for these dynamic movements.
McGill described the spine as a ‘fishing rod’ with the core intrinsic muscles as the ‘guy-wires’ to provide a preparatory compressive load to the lumbar spine in order to transmit forces through the trunk. Lumbar facet joints similar to the sacroiliac joint (SIJ) contribute a few degrees of rotation at each segment due to their highly congruent joint surfaces. Intervertebral disks made up of the annulus fibrosus and nucleus pulposus ensure the compressive force on the spine is dampened to stress-shield the bony structures. Coupled motion, first described by Lovett in 1903, ensures the load is not only distributed among the tissues but also aids in locomotion and movement. As the lumbar spine extends, it induces sacral nutation which tenses the strong sacrotuberous, sacrospinous, and interosseous ligaments enhancing pelvic stability. The iliolumbar ligament helps to stabilize the lumbar spine against trunk flexion and side flexion in the other directions of movement. Physiologic coupling occurs at the L5-S1 junction where the sacrum side bends and rotates opposite and L5 counterrotates off the sacrum.
The pelvis was described as the ‘hub’ of force transfer from the ground to the trunk and vice versa by Lovejoy in 1988. Sufficient mobility is needed at the SIJ for the intrapelvic forces to be distributed efficiently up and down the kinetic chain. That said, due to the SIJ’s inherent stability with large ligamentous support and lumbodorsal fascia overlay, there is very little movement within the joint. As load increases, the SIJ undergoes force closure to allow for maximum stability while the erector spinae and multifidus contract to stabilize the lumbar spine and pull the ilia toward each other to enhance the force closure. Repetitive asymmetric loading through the SIJ is commonly seen in baseball, which can create asymmetric adaptations to SIJ orientation and mobility. Appropriate assessment is needed to identify these impairments early in order to mitigate potential stress risers either at the SIJ or above and below.
Timing of the SIJ force closure and coupling motions of the spine is critical. Gracovetsky theorized that human movement begins with the lumbopelvic junction followed by movement of the extremities. In order for a pitcher or hitter to advance toward their target, the lumbar spine must first side-bend away and rotate toward their target. This coupled motion will help advance the acetabulum toward the target. The preparatory movement and thus stabilization of the core and pelvis allows for a potential energy to travel down the stance leg imparting kinetic energy into the ground (ie, ground reaction forces) that travel back up the kinetic chain to advance the center of mass toward the target. The same process is true on the landing leg of the pitcher or hitter summating ground reaction forces through proper sequencing of proximal to distal segments in order to translate energy from the frontal plane into the transverse plane for maximum output. Inefficient energy transfer either through improper skill mechanics or movement dysfunction from immobility or poor stability can impede performance and also lead to pathology.
Pitching
Pitching mechanics and their relation to performance and health are one of the most studied topics in sports medicine and biomechanics. Baseball pitchers have demonstrated to have the highest angular velocities in all of sports. Throwing a pitch is a combination of strength, mobility, and movement efficiency that produces elite power and velocity. There is a requisite need for mobility and stability through the kinetic chain energy transfer for success. Combine that with competing on an uneven surface not replicated in sports and you will see unique physical adaptations rarely related in other sports. Regardless of throwing from wind-up or stretch, every pitch begins standing at rest with the spine erect and the head over the hips. From here, the torso and pelvis must flex, rotate, extend, and side-bend leading to total motion toward ball release at home plate. There are almost 60° of rotation range of motion and angular acceleration over 7000° per second.
Pitchers seek to improve performance with higher throwing velocity. Peak ground reaction forces have been shown to correlate with pitching velocity. This would suggest that efficient energy transfer from the ground through the lumbopelvic region to the throwing hand can lead to health and success. During pitch mechanics, trunk muscles do not work in isolation. There is a balance of co-contraction as well as firing patterns during the rapid acceleration from a resting position that is required to complete the pitching motion. Trunk lordosis is controlled through eccentric contraction of hip and spine flexors as well as thoracolumbar fascia in anticipation of force generation. Appropriate timing of this mechanism becomes paramount when considering the efficient transfer of forces through the kinetic chain. We have known since Toyoshina’s work in 1974, that half of the kinetic energy and force production during the entire throwing motion is attributed to the trunk.
Hitting
Hitting a baseball has been described as the most difficult task in all of sports. Pitch velocities reaching over 100 miles per hour create the need for split-second decision-making. Similar to pitching, hitting a baseball begins with a static posture in a ready position. When the decision to swing is made, a series of events creating a transfer of incredible energy from the ground up must occur to complete the swing and connect with power. Maximum trunk rotation averaging 46° and an angular velocity over 7000° per second demonstrate the high stress placed on the abdomen and spine. The end of pelvic rotation occurs at the midpoint of the swing and creates abdominal elongation, which transitions to upper trunk rotational force to impact the pitch. Interestingly, the moment of highest torque in a baseball swing is during follow-through immediately after ball contact.
Game play
Delivering and hitting a pitch are 2 actions unique to baseball, but represent only a fraction of overall game play that leads to demand on a player. While the rotational acceleration component leads to the higher correlation to lumbopelvic issue, other factors must be considered. Even with new rules in place to increase the overall pace of play, game times still average over 2 and a half hours creating a large time-on-feet demand.
Freeston and colleagues showed that defensive workloads can be different per position. For example, outfielders spend more total time running, and running at high speeds, compared to other positions. This includes making plays on balls hit to them, backing up plays to other parts of the field, and running in and out of the dugout to their position between innings. First baseman and outfielders have many hard accelerations due to the need for quick reactions and being involved in a high percentage of plays. Finally, middle infielders also have a larger percentage of accelerations, but they uniquely make more total throws and more intense throws across the diamond. Middle infielders also often throw from different arm angles and with their momentum moving in different directions. This can lead to increased and changing stresses on the lumbopelvic region.
Player assessment and program development
Most baseball seasons, regardless of the level of play, begin with a routine health physical. Performance-based assessments that include range of motion and strength testing have become increasingly prolific. Joint range of motion including shoulder, elbow, and hip have been shown to be worth noting and monitoring for injury prediction. Lumbopelvic mobility and strength testing have also become synonymous with assessments and having a better understanding of player readiness to perform. Plank tests for time as well as stability testing with an inclinometer have been used to quantify core strength. Single-leg balance, Y-balance testing, and the functional movement screen have also been used. Assessment of static posture can also be useful to note morphologic changes through single and multiple seasons. Strength and conditioning coaches use counter movement jumps and mid-thigh pulls for assessment of power and strength. Qualitative reassessments can help provide insight to the temporal changes in alignment, mobility, and stability of the pelvis and spine. These are all useful measures to use as comparative baselines at incremental timepoints through the season and are key pieces of a successful program. The authors acknowledge and support the use and interpretation of these tests but, for the purposes of this article, look to address injury prevention and day-to-day readiness of a player.
Impact of assessment on game play
High rotational velocity requirements, if not timed properly, can lead to muscle strain and more. Poor core stability can lead to increased lordosis at maximal shoulder external rotation causing decreased energy transfer and more local stress leading to low back pain. In pitchers, those with better lumbopelvic control performed better than their counterparts in certain metrics (more innings pitched and fewer walks per inning). Tsao and colleagues noted poor neuromuscular control is a predisposing factor that results in low back pain. Therefore, we believe that some of the factors leading to low back pain can be both prevented and treated to maximize game performance and minimize time loss.
Daily assessment consideration
A baseball game presents an unpredictable workload by nature. Some games require more time on feet, hard accelerations, and high-end sprints compared to others. Game play that includes extreme range of motion and high tissue forces creates a constantly changing clinical presentation. Moreover, team travel including long periods of sitting and inconsistent sleep schedules can also take their toll on player presentations. Monitoring acute changes to joint mobility, soft tissue pliability and extensibility, and core stability can create a daily plan to prepare for that day’s activity.
The busy nature of the athletic training room, as well as overall daily schedule commitments, demands a quick, easy, but effective assessment process to determine what interventions can return a player to baseline presentation and optimize their ability to continue playing at a high level. Many tests and measurements have been described in the literature for core strength assessments such as McGill stability test, plank test, trunk extension endurance test, and many other tests of stability and stamina. However, it is the opinion of the authors that the consistent use of these tests can lead to unnecessary fatigue that can affect capacity for training and game play. Also of note, while muscle endurance is important, it does not necessarily predict sports performance. Additionally, in high-velocity rotational athletes, there may be a pulsing effect to co-contraction of the core musculature allowing for both trunk and pelvis stabilization while maximizing rotational angular velocity. Thus, both the speed of contraction and the speed of relaxation are necessary.
A quick assessment of mobility and function is needed to help make treatment plan decisions. The authors’ suggestion is described in the following sections. The authors recommend a multidisciplinary approach clustering all evidence toward developing a care plan taking into consideration evidence-based practice, clinician experience and expertise, as well as player opinion and feedback.
Assessment begins with overall alignment with static posture and moving into the following sequenced assessment:
- •
Joint alignment and range of motion
- ○
Long sit test alignment test
- ○
ASIS equilibrium assessment–standing/supine
- ○
Sacroiliac joint assessment
- ▪
Joint orientation and axis of rotation
- ▪
- ○
Lumbar spine segmental assessment
- ▪
Posterior to anterior segmental accessory mobility assessment
- ▪
Passive physiologic intervertebral motion
- ▪
- ○
Femoral-acetabular joint mobility assessment
- ▪
Supine–lateral, inferior, lateral/inferior oblique
- ▪
Prone–anterior
- ▪
- ○
- •
Muscle function assessment
- ○
Supine single leg hip abduction isometric
- ○
Prone hip extension isometric at 0 abduction
- ○
Prone hip extension isometric at 30 abduction
- ○
Sacroiliac assessment in regards to alignment, mobility, and stability
Qualitative assessment involves clustering of multiple movement testing to identify impairment(s). Cibulka showed high reliability of clustering of innominate dysfunction tests to identify SIJ dysfunction. Standing trunk mobility assessment involves assessing the posterior superior iliac spine (PSIS) excursion during similar movements during the snapshot triplanar static posture pictures. The Stork test (Gillet test) requires palpation of the inferior aspects of the PSIS (moderate to good reliability). Typically, the PSIS will move inferior with contralateral leg raise. If the PSIS remains level or moves superiorly, it warrants further evaluation of the SIJ. Using the same inferior PSIS landmark, standing flexion will incur superior migration of the PSIS during trunk flexion. Abnormal movement unilaterally or excessive superior migration is noted. The seated flexion test is also used in the same manner. During trunk extension, the examiner is assessing for asymmetry and unexpected movement of the PSIS.
The supine to long sit test (Weber-Barstow test) is a common technique used to assess pelvic alignment and possible iliosacral dysfunction. Side-to-side changes in leg length presentation from supine to sit can be indicative of a change in sacral nutation or rotation of the innominate. The presence of a leg length discrepancy has been shown to increase the load across the SIJ 5-fold. Using the inferior aspect of the medial malleoli as anatomic landmark comparing bilaterally, the examination involves the following steps.
- •
Lay supine.
- •
Assess malleolus evenness.
- •
Actively bend knees into a resting bridge position and complete 2 bridges.
- •
Return to the long leg supine position.
- •
Reassess malleoli levels by comparing bilaterally.
- •
Ask the athlete to come to a long sit position and return to laying supine.
- •
Note any changes to malleolus evenness.
Supine ilium (innominate) mobility is assessed by providing an anterior to posterior pressure to the anterior superior iliac spine in the oblique plane (in line with the SIJ). In prone, the same joint mobility assessment can be done via a posterior to anterior pressure to the sacral base, mid-sacral body, and inferior lateral angle. Noting asymmetrical mobility excursions combined with the supine to sit test, Gillet test, and standing trunk range of motion test can help the clinician identify a malalignment of an innominate and/or mobility restriction of the SIJ.
The active straight leg raise test can further help elucidate lumbopelvic motor control dysfunction. The test is performed in supine position by flexing the ipsilateral hip to roughly 20 cm. Without appropriate core abdominal bracing during the test, an anterior rotation of the ilium will occur.
Spinal segmental assessment in regards to postural alignment, mobility, and stability
Lumbar assessments of segmental derangement or hypomobility have varying evidence of inter-rater reliability to support its use. However, a 3-dimensional (3-D) approach should include functional movement, stability, and pelvic alignment and mobility. It is the opinion of the authors that the clinical significance of intra-rater findings of these assessments cannot be ignored. Lumbar segmental mobility is assessed either via passive accessory intervertebral motion or through passive physiologic intervertebral motion (PPIVM) described by Maitland. Accessory mobilization is done in prone via a posterior to anterior glide on the transverse processes in line with the facet joints. PPIVM is performed in the hook-lying position utilizing a lumbar lock below the segment of mobilization by flexing the hips till the spinous process of the inferior segment moves into flexion. Then, the clinician provides a thoracic rotation via the ribcage as the fulcrum. In addition, lumbar side flexion can be assessed in the same hook-lying position by again locking the segment below and raising the lower legs to induce side bend from below. The clinician notes asymmetric mobility and clusters the standing trunk mobility testing to confirm the specific segment of restriction.
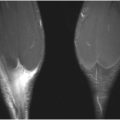
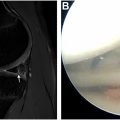
Isolated clinical assessments for core stability can help elucidate motor control deficits. One such assessment that can be quickly utilized is the Sahrmann core stability test. Level 3 of the 5-level test is performed in supine position with both the hips and knees flexed to 90° and slowly lowering 1 leg to roughly 12 cm above the ground or table ( Fig. 1 ). Inability to maintain lumbopelvic stability is a sign that the transverse abdominis, rectus abdominis, and internal and external obliques may not be co-contracting synergistically to stabilize the lumbopelvic junction. Another efficient clinical assessment to evaluate multifidus activation is the multifidus lift test. In prone, the athlete’s shoulders are placed in 120° of flexion with 90° of elbow flexion and the athlete is asked to raise their arm toward the ceiling to approximately 5 cm above the ground or table while the clinician palpates their contralateral lumbar multifidus. Side-to-side differences can be appreciated by palpating for a firm muscle contraction. A variation of this test that the current authors’ utilize is a slight prone leg lift while palpating the contralateral multifidi ( Fig. 2 ).