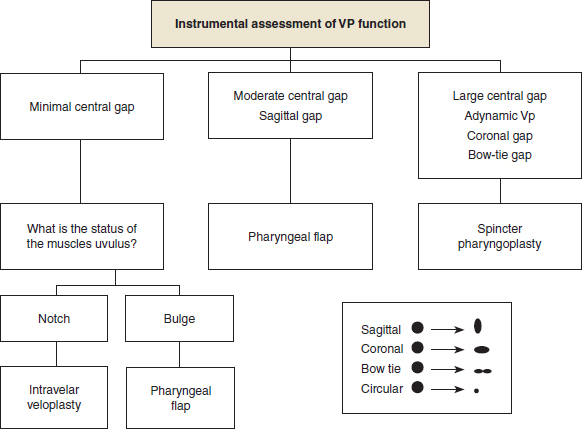
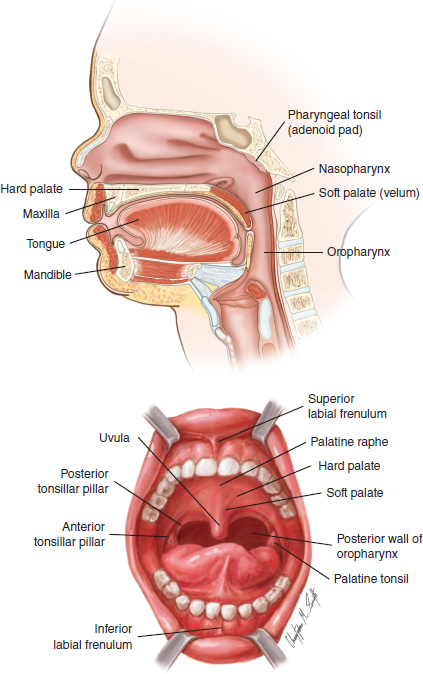
60 ○ Ideal management of velopharyngeal dysfunction will normalize resonance, eliminate nasal turbulence, and improve articulation while maintaining patency of the nasal airway. ○ Velopharyngeal dysfunction may have multiple causes, and surgical intervention should be matched to the specific problem. ○ Sphincter pharyngoplasty is one surgical approach to velopharyngeal dysfunction that often yields good results in patients with impaired lateral pharyngeal wall motion as documented on diagnostic endoscopic and radiographic imaging. ○ Our preferred sphincter pharyngoplasty technique uses superiorly based myomucosal flaps that include the palatopharyngeus muscles. ○ The myomucosal flaps are transposed and interdigitated at the posterior pharyngeal wall at the level of the first cervical vertebra, creating a small central port. ○ Excellent results can be anticipated in appropriately selected patients. Inability to completely separate the nasal cavity from the oral cavity for required speech tasks (velopharyngeal dysfunction) results in a verbal communication impairment that can range from minor speech distortion to unintelligibility.1 Once such an impairment is recognized, evaluation and management may involve speech-language pathologists, endoscopists, radiologists, prosthodontists, surgeons, and geneticists, usually in the context of a cleft palate team.2 Members of these health care disciplines may even work as an interdisciplinary velopharyngeal team. The discussion of a holistic approach to velopharyngeal dysfunction evaluation and management is the subject of other chapters in this text; this chapter reviews velopharyngeal anatomy and hypotheses regarding velopharyngeal dysfunction management in relation to one specific surgical technique for velopharyngeal dysfunction: sphincter pharyngoplasty. The velopharynx is a space bounded in the axial plane (horizontally) by soft tissues, which usually are capable of approaching each other through the dynamism of underlying muscles, and in the sagittal plane (superiorly and inferiorly) by spaces (Fig. 60-1). The axial plane soft tissues are the velum (soft palate) anteriorly, the posterior pharyngeal wall posteriorly, and the right and left lateral pharyngeal walls laterally. The superior and inferior spaces include the nasopharynx superiorly and the oropharynx inferiorly. The velopharynx is often referred to as either a sphincter, emphasizing the normal dynamism of the surrounding myomucosal tissues, or a port, emphasizing the space connecting the nasal and oral pharynges. The normally functioning velopharynx is usually fully patent, allowing unencumbered airflow between the nasal and oral cavities and free drainage of nasal secretions into the throat, except during swallowing and specific speech tasks when contraction of its surrounding muscles separates the nasal cavity from the oral cavity. With respect to speech, a malfunctioning velopharynx is characterized by one or more of the following: hypernasality (excessive or inappropriate nasal resonance), nasal turbulence, and facial grimacing. Fig. 60-1 Anatomy of the velopharynx. The basic hypothesis regarding velopharyngeal dysfunction management is that modification of the velopharyngeal port will improve velopharyngeal function for speech. Specifically, velopharyngeal dysfunction management will normalize resonance, permitting secondary elimination of velopharyngeal dysfunction-associated malarticulations with speech therapy. In addition, velopharyngeal dysfunction management will eliminate nasal turbulence and facial grimacing. Maintenance of patency of the nasal airway for breathing and secretion control generally has not been a component of the basic management hypothesis. The primary morbidity of an unrepaired cleft palate is impaired speech intelligibility. This impairment usually compromises self-image, education, employment, and socialization. In the mid-nineteenth century, elimination of the overt palatal defect was hypothesized to resolve the functional problems associated with cleft palate. However, the inability of successful static anatomic repair of cleft palate to consistently eliminate speech impairment was appreciated by at least the first quarter of the twentieth century. This led to the second major cleft palate repair hypothesis: Increased velar length will improve speech intelligibility. Surgical techniques designed to lengthen the palate can be grouped as (1) those that include dorsal displacement of the mucoperiosteum of the hard palate in an attempt to dorsally displace the soft palate (often referred to as palatal pushback) and (2) those that only attempt to increase the length of the soft palate directly. Although rigorous validation of either of these types of operations to consistently improve velopharyngeal function is lacking, multiple purported validations have been published over the past several decades. By the 1920s, some cleft surgeons hypothesized the importance of dynamism rather than the amount of palatal tissue as the critical variable in velopharyngeal function. Two categories of operations were proposed to optimize such function: (1) reconstruction of the intravelar muscular sling and (2) reorientation of the lateral pharyngeal wall musculature, specifically the palatopharyngeus muscles. Intravelar veloplasty, the generic name of the first of these categories, became a standard component of primary palatoplasty by the 1970s and subsequently has been advocated by some as the preferred initial technique to manage postpalatoplasty velopharyngeal dysfunction.3 More recently, increasing velar length and velar muscle reorientation have been combined as the Furlow double-opposing Z-plasty.4 An alternative approach to velopharyngeal dysfunction management focused on obstruction of the excessively patent velopharyngeal port during physiologic tasks when it failed to close sufficiently. Obstruction of the velopharyngeal port can be either completely reversible using a prosthetic device (palatal lift, obturator, or lift-orator) that is only worn during the day for speech or with a permanent subtotal surgical obstruction that only can be reversed with another operation.5,6 Such obstructive operations result either in a diminished single central velopharyngeal port (posterior pharyngeal wall augmentation and sphincter pharyngoplasty) or two laterally placed ports (pharyngeal flap). Diminution of the cross-sectional area of the velopharyngeal port can introduce a new morbidity not associated with other attempts at eliminating velopharyngeal dysfunction, sufficient obstruction of the nasal airway to impair both breathing (causing mouth breathing or obstructive sleep apnea) and hygiene (nasal secretion retention and stasis).7–9 No operation, whether a component of primary palatoplasty or a specific intervention for velopharyngeal dysfunction, can normalize velopharyngeal function for speech, swallowing, and breathing in all patients. We, among other surgeons, have differentiated treatment for velopharyngeal dysfunction based on differential diagnosis. This approach assumes that one specific intervention will not be successful in normalizing resonance and maintaining a patent nasal airway for all patients regardless of the cause of the velopharyngeal dysfunction. Rather, it assumes that specific causes of velopharyngeal dysfunction require specific matched interventions. Some studies have attempted to test this hypothesis.10–12 Wilfred Hynes13 pioneered the use of pharyngoplasty to treat velopharyngeal incompetence in cleft palate patients. He initially published his pharyngoplasty technique in 1950, emphasizing that any pharyngoplasty procedure to treat what he termed the “failed cleft patient” should reduce the transverse diameter of the pharynx and shorten the anterior-posterior dimension by creating a ledge of tissue higher than Passavant’s ridge. He also stressed the importance of preserving viable muscle, leaving the superior constrictor muscle undisturbed and creating a tension-free repair. His two-stage technique, as described in his 1950 publication, called for elevation of bilateral, superiorly pedicled myomucosal flaps based on the small salpingopharyngeus muscle. These flaps were elevated up to the level of the Eustachian cushion and then inset into a high, transverse mucosal defect in the posterior pharyngeal wall, overlapping the flaps “significantly.” The donor sites were then closed, further narrowing the cross-sectional area of the pharynx. The palate was closed in a pushback procedure months later to complete the pharyngoplasty. Although Hynes’ initial article advocated the use of only the salpingopharyngeus muscle and its overlying mucosa, his 1953 Hunterian lecture to the Royal College of Surgeons in England modified his original procedure to include elevation of the palatopharyngeus muscle with the salpingopharyngeus, adding significant muscular bulk to the repair.14 This modification was, no doubt, a reflection of his recognition that patients with cleft palate who have velopharyngeal insufficiency and poor speech results often have both a deep, large pharynx and a short, scarred palate—in essence, both a cross-sectional area problem and a movement problem. By adding more muscular bulk, he presumably hoped not only to create a larger ridge than the salpingopharyngeus was capable of providing but also to create a more robust, dynamic flap. More than a decade later, Miguel Orticochea popularized pharyngoplasty for the management of velopharyngeal problems in patients with clefts. Although some have characterized Orticochea’s dynamic muscle sphincter as a modification of Hynes’ procedure, others have disagreed with that assertion (see accompanying discussion by Lendrum).15 Orticochea’s 1968 paper16 describing his technique focused far more on achieving sphincterlike function to aid speech than on changing the depth or cross-sectional area of the pharynx as advocated by Hynes. Orticochea’s technique as originally described required closure of the palate as a first stage. Then, 6 months later, the posterior tonsillar pillars were transplanted to the midline of the posterior pharynx. The flaps were inset into a small, inferiorly based pharyngeal flap, sufficiently large to allow transplantation without tension. Flaps were sewn not only to the small pharyngeal flap but also to each other to minimize the risk of dehiscence. At the conclusion of the operation, three openings remained to conduct air between the oral and nasal pharynx: a central opening between the two muscle flaps and two lateral openings that contract and ultimately close as they heal. As previously noted by others, Orticochea’s technique “ignored the normal closure mechanism and has itself been modified subsequently.”15,17–20 Whether Orticochea’s dynamic muscle sphincter is considered a modification of Hynes’ procedure or a philosophically different approach to the same problem is irrelevant. The many modifications of Orticochea’s original pharyngoplasty description have yielded a contemporary pharyngoplasty procedure that very much mirrors that described much earlier by Hynes. As already noted, we use the differential diagnosis of velopharyngeal dysfunction to determine the specific treatment offered to an individual patient. Whereas auditory perceptual speech evaluation can identify velopharyngeal dysfunction and document associated speech impairments, listening to speech cannot identify the pathophysiology of the velopharyngeal dysfunction, even when the listener is a speech-language pathologist well experienced in velopharyngeal dysfunction. Furthermore, instrumental velopharyngeal assessments that indirectly measure changes in the velopharyngeal port during function (aerodynamics, nasalance) cannot delineate the pathophysiologic basis of the velopharyngeal dysfunction. Imaging of velopharyngeal function, either nasendoscopically or fluoroscopically, can define which of the velopharyngeal components is malfunctioning.21 My (JLM) preference, based on 35 years of clinical experience with velopharyngeal management, is to use sphincter pharyngoplasty specifically for the surgical treatment of those patients whose velopharyngeal dysfunction is secondary to markedly impaired or absent lateral pharyngeal wall motion22 (Fig. 60-2). I adopted this approach after becoming familiar with sphincter pharyngoplasty in 1989, because these patients require a wide obstructive flap when managed with a pharyngeal flap, which is usually associated with significant impairment of the nasal airway. Although sphincter pharyngoplasty also can impair the nasal airway, the magnitude of the morbidity has been less than that with wide obstructive pharyngeal flaps in my practice.7,8
Sphincter Pharyngoplasty
Jeffrey L. Marsh, Earl A. Gage
KEY POINTS
ANATOMY OF THE VELOPHARYNX
BASIC VELOPHARYNGEAL DYSFUNCTION MANAGEMENT
CLEFT PALATE REPAIR AND VELOPHARYNGEAL FUNCTION
HISTORY AND EVOLUTION OF THE SPHINCTER PHARYNGOPLASTY PROCEDURE
INDICATIONS FOR SPHINCTER PHARYNGOPLASTY
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine