The anatomic region influences the dermoscopic features of different lesions. In this article, the particular characteristics of the scalp, mucosal membranes, and lesions located on the milk line are explained. In histopathology, the benign melanocytic lesions in these locations are also named nevi of special sites, considering the difficulty of the histopathologic diagnosis.
Key points
- •
The anatomic region influences the dermoscopic features of lesions, resulting in specific criteria that help make correct management decisions for lesions located on the scalp, mucosal membranes, and milk-line and in flexural locations.
- •
Biopsy should be performed in lesions of the scalp if atypical pigment net or pseudopigment net in association with regression areas is present, if a homogeneous blue lesion lacks a convincing subjective history of no changes, and if there is a growing nodular tumor. Regular globular pattern and reticular pattern with central hypopigmentation (eclipse nevus) are most common in melanocytic nevi on the scalp of children and young adults.
- •
In mucosal lesions with diameter larger than 1 cm, gray color and the presence of structureless areas are highly suggestive for mucosal melanoma, whereas one color and regular dermoscopic structures are the main criteria of benign mucosal melanosis.
- •
Nevi located on the milk line and in flexural locations, such as axilla, inguinal region, popliteal, and antecubal fossa, can frequently display a prominent pigment net, sometimes with bizarre lines, and large globules mimicking features of melanoma.
Lesions on the scalp
A high concentration of pilosebaceous follicles and rich vascular and lymphatic supply form the special anatomic appearance of the skin of the scalp. Scalp tumors account for approximately 2% of all skin tumors and may derive from different cell types of the pilosebaceous unit, from the interfollicular epidermis and dermis, or as cutaneous metastases from other tumors.
The great variety of scalp tumors consists of sebaceous nevus, seborrheic keratosis, basal cell carcinoma, actinic keratosis, squamous cell carcinoma, hemangioma, angiosarcoma, and rare adnexal tumors. The dermoscopic appearance of these tumors normally does not differ from that on other body sites. Thus, this article concentrates on melanocytic lesions.
Melanocytic scalp tumors differ in some epidemiologic, morphologic, and biologic aspects from their counterparts on the trunk. For example, scalp melanoma has a poorer prognosis compared with thickness-matched melanomas of the trunk. Blue nevi are more frequently found on the scalp than on other body sites and histopathology of some melanocytic nevi may simulate melanoma.
Melanocytic Nevi
The prevalence of nevi of the scalp in children is approximately 10%. The morphology of nevi of the scalp changes according to the age of patients, and older people more frequently show less pigmented papillomatous nevi.
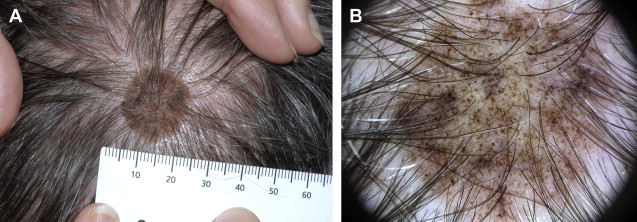
Large congenital nevi involving the scalp should always lead to a screening for neurocutaneus melanosis. Dermoscopy is not helpful in deciding further management of congenital nevi, especially those located on the scalp. In this location, hairs make an investigation of nevi sometimes impossible. The threshold for excision should be low ( Fig. 1 ).
Scalp nevi in children may be a source of anxiety for parents. Clinically, these nevi can display large size, irregular borders, and color variation. Frequently, these nevi appear in the first years of live. Because of the sometime worrisome clinical appearance and the anxiety of parents, these nevi are unnecessarily excised. In their study, Tcheung and colleagues described 4 different clinical patterns of scalp nevi in children: homogeneous brown (48%), solid pink (28%), eclipse (21%), and cockade (3%). The predominant dermoscopic feature was globules, which was found in 57% of scalp nevi as the only dermoscopic feature. In addition, 27% of scalp nevi showed a combination of globular and reticular patterns. Only 9% of the nevi showed solely a reticular pattern, followed by 6% showing a homogenous pattern.
Perifollicular hypopigmentation was seen in the majority of nevi. This finding was confirmed in a study by Stanganelli and colleagues. In this study, the investigators studied 323 excised tumors of the scalp (including 78 melanocytic nevi and 21 blue nevi) from 315 patients (mean age 52 years; range 3–88 years); 48% of melanocytic nevi were found to display hypopigmentation, which was perifollicular in 15 cases and central in 14. Perifollicular hypopigmentation was also present at the border of lesions, resulting in an irregular shape.
Because excision was an inclusion criterion of this study, the percentage of linear irregular vessels was surprisingly high in this sample. In the author’s experience, the main vascular pattern in scalp nevi is comma vessels and dotted vessels.
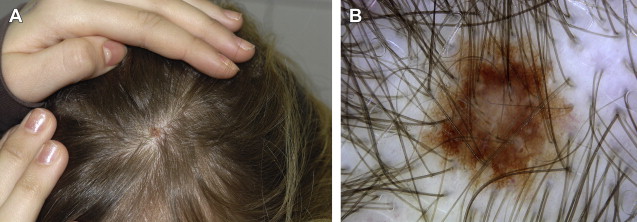
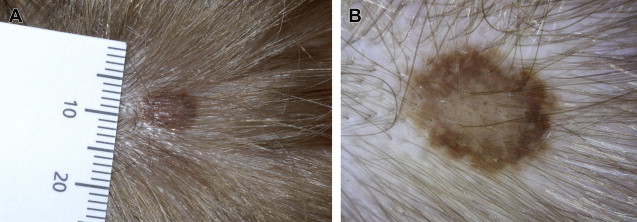
Clinically, scalp nevi in children and adolescents present as macule or flat nodule with homogeneous pink or brown color. Most of the lesions on the scalp are symmetric. Dermoscopy normally reveals a globular pattern, perifollicular hypopigmentation, and central hypopigmentation (eg, eclipse nevus) ( Figs. 2 and 3 ), whereas most scalp nevi in adults are usually nodular and faint pigmented or skin colored with a smooth or papillomatous surface. Comma vessels and dotted vessels are found by dermoscopy ( Figs. 4 and 5 ). All these lesions can be managed conservatively, because there is no documented risk for malignant transformation.
Small congenital nevi with asymmetry and multiple colors or nevi displaying melanoma-specific criteria should be excised.
Blue Nevus of the Scalp
Blue nevi are common on the scalp and may develop at any age. Clinically, blue nevi present as flat to prominent blue nodules with a smooth surface. In most cases, the diameter is smaller than 1 cm but giant congenital forms are also described. Once developed, they do not change over a long time period.
The homogeneous blue pattern is the stereotypical dermoscopic pattern of blue nevi, and lesions on the scalp are not an exception ( Figs. 6 and 7 ). In their study, Stanganelli and colleagues included 27 blue nevi, which showed in 89% a homogenous blue pigmentation and in almost half the cases areas of hypopigmentation. In contrast to blue nevi located on other body sites, the investigators found in 8 blue nevi on the scalp an atypical vascular pattern (ie, linear irregular vessels [see Fig. 6 ]). This might be due to the rich vascular supply of the scalp.
Variants of blue nevi, such as deep penetrating blue nevus and so-called malignant blue nevus, which represents a variant of nodular melanoma in the eyes of some investigators, seem more frequent on the scalp than on other body sites. In a retrospective histopathologic study of 23 malignant blue nevi, 6 tumors were located on the scalp and the prognosis did not differ from matched melanomas of the same thickness.
Moreover, nodular melanoma, cutaneous metastases of melanoma, and heavily pigmented basal cell carcinoma can be indistinguishable from blue nevi. The history of change and growth is sometimes the only criterion, which can lead to the correct diagnosis of a malignant tumor. Thus, it is has been recommended to excise blue lesions on the scalp, if there is not subjective history of a stable lesion over years.
Melanoma of the Scalp
Melanoma and nonmelanoma skin cancer of the scalp are most frequent in bald men aged over 65 years. Frequently, signs of chronic sun damage and previous history of skin cancer are found in patients developing a melanoma on the scalp. These data support that UV irradiation plays a role in their pathogenesis.
Lentigo maligna, lentigo maligna melanomas, superficial spreading melanomas, and nodular, fast-growing melanomas can be differentiated.
Generally, the dermoscopic features of melanomas on the scalp do not differ from those on other body sites.
On bald skin, lentigo maligna and lentigo maligna melanomas display the characteristic features of asymmetric pigmented hair follicles, gray dots and globules, and occlusion of the hair follicles. The association with actinic keratosis or other nonmelanoma skin tumors can obscure the diagnosis. Moreover, the differentiation of lentigo maligna from a solar lentigo may be difficult ( Fig. 8 ). Brown color, sharp moth-eaten borders, and fingerprint-like structures favor the diagnosis of solar lentigo, whereas gray color, diffuse border, and asymmetric hair follicles are suggestive of lentigo maligna.
Most cases of superficial spreading melanoma on the scalp display the typical dermoscopic features of melanoma and can be diagnosed easily. Asymmetry and more than 3 colors together with melanoma-specific local criteria are found in melanomas on the scalp at a similar frequency as in melanomas on other anatomic sites. Atypical network or brown-gray pseudonetwork and regression were found predictive for thin (<1-mm) melanomas ( Fig. 9 ).
Thick, fast-growing, nodular melanoma often lacks specific dermoscopic patterns ( Fig. 10 ). The homogenous blue and or black nodules frequently resemble blue nevi, heavily pigmented basal cell carcinoma, or metastatic melanoma. Sometimes irregular, polymorphous vessels can be a hint for malignancy of a given tumor. Irregular black blotches or dots over a blue background may be an important clue for diagnosis. Black blotches and dots were absent in 26 of 27 blue nevi in an International Dermoscopy Society study. Usually the history of rapid growth makes excision mandatory.
Amelanotic or hypomelanotic nodular melanoma can mimic pyogenic granuloma, the main dermoscopic features of which are a white collarette and white thick lines (white rail lines). When pyogenic granuloma is removed, histology is obligatory to exclude melanoma.
Summary: Melanocytic Lesions on the Scalp
Total body skin examination should include the scalp.
Melanocytic nevi of the scalp show age-related changes in the their dermoscopic appearance. While scalp nevi in children and young adults typically exhibit a globular or reticular pattern with central hypopigmentation (eclipse nevus), scalp nevi in older persons tend to be raised, papillomatous and hypopigmented or skin colored (intradermal nevus).
Blue nevi should be excised except when there is a history of an unchanged, stable lesion.
Atypical pigment network or pseudopigment network in association with regression areas is indicative for thin melanomas on the scalp.
A biopsy should be performed in lesions with prominent regression because differentiation of lichen planus–like keratosis, regressing seborrheic keratosis, and pigmented actinic keratosis from melanoma may be difficult.
Thick nodular melanomas are sometimes indistinguishable from blue nevi, pigmented basal cell carcinoma, pyogenic granuloma, and metastatic melanoma; thus, growing nodular lesions have to be excised without exception.
Lesions on the scalp
A high concentration of pilosebaceous follicles and rich vascular and lymphatic supply form the special anatomic appearance of the skin of the scalp. Scalp tumors account for approximately 2% of all skin tumors and may derive from different cell types of the pilosebaceous unit, from the interfollicular epidermis and dermis, or as cutaneous metastases from other tumors.
The great variety of scalp tumors consists of sebaceous nevus, seborrheic keratosis, basal cell carcinoma, actinic keratosis, squamous cell carcinoma, hemangioma, angiosarcoma, and rare adnexal tumors. The dermoscopic appearance of these tumors normally does not differ from that on other body sites. Thus, this article concentrates on melanocytic lesions.
Melanocytic scalp tumors differ in some epidemiologic, morphologic, and biologic aspects from their counterparts on the trunk. For example, scalp melanoma has a poorer prognosis compared with thickness-matched melanomas of the trunk. Blue nevi are more frequently found on the scalp than on other body sites and histopathology of some melanocytic nevi may simulate melanoma.
Melanocytic Nevi
The prevalence of nevi of the scalp in children is approximately 10%. The morphology of nevi of the scalp changes according to the age of patients, and older people more frequently show less pigmented papillomatous nevi.
Large congenital nevi involving the scalp should always lead to a screening for neurocutaneus melanosis. Dermoscopy is not helpful in deciding further management of congenital nevi, especially those located on the scalp. In this location, hairs make an investigation of nevi sometimes impossible. The threshold for excision should be low ( Fig. 1 ).
Scalp nevi in children may be a source of anxiety for parents. Clinically, these nevi can display large size, irregular borders, and color variation. Frequently, these nevi appear in the first years of live. Because of the sometime worrisome clinical appearance and the anxiety of parents, these nevi are unnecessarily excised. In their study, Tcheung and colleagues described 4 different clinical patterns of scalp nevi in children: homogeneous brown (48%), solid pink (28%), eclipse (21%), and cockade (3%). The predominant dermoscopic feature was globules, which was found in 57% of scalp nevi as the only dermoscopic feature. In addition, 27% of scalp nevi showed a combination of globular and reticular patterns. Only 9% of the nevi showed solely a reticular pattern, followed by 6% showing a homogenous pattern.
Perifollicular hypopigmentation was seen in the majority of nevi. This finding was confirmed in a study by Stanganelli and colleagues. In this study, the investigators studied 323 excised tumors of the scalp (including 78 melanocytic nevi and 21 blue nevi) from 315 patients (mean age 52 years; range 3–88 years); 48% of melanocytic nevi were found to display hypopigmentation, which was perifollicular in 15 cases and central in 14. Perifollicular hypopigmentation was also present at the border of lesions, resulting in an irregular shape.
Because excision was an inclusion criterion of this study, the percentage of linear irregular vessels was surprisingly high in this sample. In the author’s experience, the main vascular pattern in scalp nevi is comma vessels and dotted vessels.
Clinically, scalp nevi in children and adolescents present as macule or flat nodule with homogeneous pink or brown color. Most of the lesions on the scalp are symmetric. Dermoscopy normally reveals a globular pattern, perifollicular hypopigmentation, and central hypopigmentation (eg, eclipse nevus) ( Figs. 2 and 3 ), whereas most scalp nevi in adults are usually nodular and faint pigmented or skin colored with a smooth or papillomatous surface. Comma vessels and dotted vessels are found by dermoscopy ( Figs. 4 and 5 ). All these lesions can be managed conservatively, because there is no documented risk for malignant transformation.




