Soft Tissue Coverage of the Knee: Free Flaps
Goo-Hyun Mun
So Young Kim
DEFINITION
Although most soft tissue and bony defects around the knee are usually covered with locoregional tissues, free flaps should be considered when the desired donor territory is damaged or unsuitable or if the defect is extensive or complex. Free flaps offer benefits such as shortened recovery time, plentiful availability of donor tissue, and greater flexibility in flap design.1
Soft tissue defects of the knee can significantly influence gait; therefore, reconstruction should be done with proper planning and technique at an early onset.2
Restoration of the thin and pliable skin for satisfactory appearance and function of the knee is an important reconstruction goal.
ANATOMY
Popliteal vessels and vessels from the anterior knee can be recipients of microvascular free flap transfer for soft tissue coverage of knee defects.
Recipient vessels for free flap.
Popliteal vessel and its branches (FIG 1A). The popliteal artery ranges from a proximal portion starting at the opening of the adductor canal to the distal portion lying behind the upper part of the tibia and fibula. The popliteal vessel and branches, including the superior medial and lateral genicular vessels (FIG 1B), medial and lateral sural vessels (FIG 1C), middle genicular vessels, and inferior genicular vessels, are considered the choice of recipient vessels for a free flap in the knee region. However, the approach to the popliteal vessels can be difficult when the anterior surface of the knee is reconstructed, and sural vessels are difficult to use in a free tissue flap to the region proximal to the knee.3 Furthermore, there is a risk of increased complications caused by compression and twisting of the flap blood vessels, depending upon the postsurgical position of the patient.
Anterior knee (FIG 2A):
Three vessels, including the descending genicular vessel and its branches (FIG 2B,C), and the descending branches of the lateral circumflex femoral vessels (FIG 2D) and anterior tibial vessels are considered the choice of recipient vessels for a free tissue transfer for the anterior knee region.
These recipient candidates have several benefits with supine positioning and easy accessibility to the recipient vessel. However, these branches may be very small vessels and, if so, may be of limited value and less reliable.3
The perforators along the intermuscular septum of the upper leg and lower thigh can be used as recipient vessels for free flap reconstruction of the knee, but also note that these vessels may be small.4
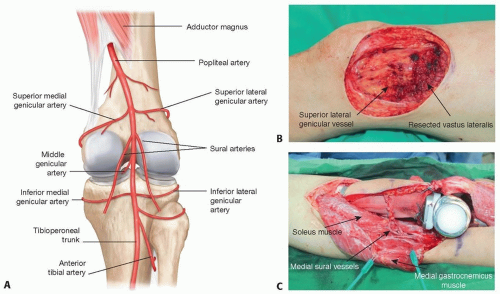 FIG 1 • A. Muscular boundaries and branches of the popliteal artery and deep neurovascular structures in the posterior knee. B. Superior lateral genicular vessel for recipient vessel. C. Medial sural vessel for recipient vessel. |
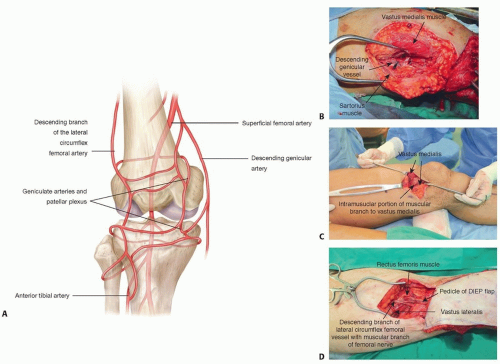 FIG 2 • A. Anatomy of recipient vessels of anterior knee region. B. Descending genicular vessels-vessel for recipient vessel. C. Descending genicular vessel-muscular branch to the vastus medialis for recipient vessel. D. Descending branch of the lateral circumflex femoral vessel for recipient vessel. |
PATHOGENESIS
Multiple prior operations and revision arthroplasties with atrophy/scarring of soft tissues
Prior coverage of a total knee prosthesis and wound dehiscence due to infection
Large post-traumatic defects
Extensive soft tissue tumor excision
Soft tissue necrosis and chronic infection after extremity radiation
Necrotizing fasciitis and septic arthritis
Burn scar contracture and post-traumatic stiff knee
PATIENT HISTORY AND PHYSICAL FINDINGS
The patient history should focus on the exact mechanism and etiology of the defect.
It is important to assess the medical history including vascular disease, systemic disease, and hypercoagulable state, which can influence the outcome of a microsurgical procedure.
The preoperative evaluation for patients with a knee defect includes a detailed assessment of function limitations. The range of motion is a widely used measure of the knee joint, with a normal range of flexion of 45 to 105 degrees during routine activities and full extension to 0 degree.5
IMAGING
The authors routinely perform preoperative computed tomography (CT) angiography of the lower extremity unless contraindicated to evaluate the regional vascular anatomy.
Magnetic resonance imaging (MRI) can also be performed for evaluation of complex defects of soft tissue.
SURGICAL MANAGEMENT
The proper selection of recipient vessels is essential for the success of a free flap and is arguably the most important factor that can affect the outcome.4,6 Major considerations regarding the choice of appropriate recipient site for revascularizing the flap include performing the microanastomosis outside the zone of injury and avoiding the need for vein grafts.7
Extending the incision from the defect is used when there is a suitable adjacent recipient; however, a separate incision with subcutaneous tunneling can be effective for a distant recipient vessel approach.
Options of free flap:
Commonly chosen flaps for soft tissue reconstruction of knee defects are an anterolateral thigh (ALT) flap, rectus abdominis muscle flap, deep inferior epigastric artery perforator (DIEP) flap, tensor fascia lata flap, superficial
circumflex iliac artery perforator (SCIP) flap, latissimus dorsi musculocutaneous flap, and thoracodorsal artery perforator (TDAP) flap. The TDAP flap is favored by the authors because of several advantages including generous dimensions of the back, tissue thinness, relatively wellhidden donor scar, a long vascular pedicle, and the versatility offered by composite tissue transfer.
When complex knee trauma accompanies a patellar tendon defect, the patellar tendon is traditionally restored using an autogenous graft, such as the semitendinosus tendon, gracilis tendon, and fascia lata, or an allograft. Because of the problem of delayed healing, fascia lata failure, and infection, a composite ALT myocutaneous flap with vascularized fascia lata can be utilized for one-stage reconstruction of complex knee defects.8
When there is post-traumatic loss of the quadriceps femoris muscles with subsequent loss of knee extension, free functional transfer of the latissimus dorsi muscle9 and contralateral rectus femoris muscle10 can be utilized to restore knee extension.
For stump coverage in above or below knee amputations, the distal placement of a flap to cover the entire weightbearing surface of the stump is required.11
TECHNIQUES
▪ Wound Preparation
The first goal of wound preparation is to debride all contaminated soft tissue or excise pathologic or necrotic lesions and to evaluate the extent of soft tissue defects in terms of size and components, including the bone, tendon, muscle, fascia, and skin (TECH FIG 1).
A tourniquet is usually applied on the thigh during wound preparation.
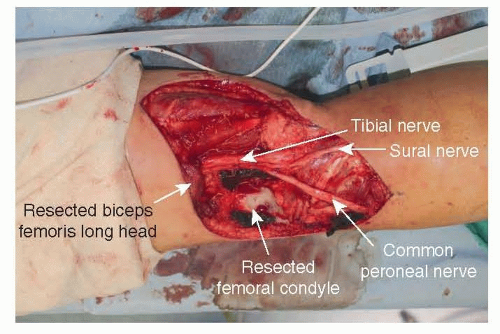 TECH FIG 1 • Wound preparation of posterior knee defect after tumor extirpation. |
▪ Recipient Vessel Preparation
Approach to the medial sural artery
The procedure can be performed with the patient in prone or semilateral decubitus position, with the recipient extremity down and the opposite leg crossed anteriorly, with simultaneous access to the contralateral back as a donor site (TECH FIG 2A).
Arising from the posterior aspect of the popliteal vessel, the medial sural vessel enters the deep surface of the medial gastrocnemius muscle. Between the muscular head of the medial and lateral gastrocnemius, the medial sural vessel is easily approached12 (TECH FIG 2B). A branch of the tibial nerve usually accompanies the dominant vascular pedicle to the gastrocnemius muscle and should be preserved.7Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Tibial Reconstruction
Tibial Reconstruction
 Reconstruction of Femur
Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


