Soft Tissue Coverage of Lower Leg—Free Flap
Goo-Hyun Mun
Kyong-Je Woo
DEFINITION
Microvascular free flap transfer is a reliable and often ideal option for soft tissue reconstruction of a complex or large wound of the lower leg.
The goal of reconstruction is to provide durable soft tissue coverage to maximize bony union in a traumatic wound and functional recovery and to restore the aesthetic contour of the lower leg.
ANATOMY
Three main arteries branching from the popliteal artery are potential recipient vessels for microvascular free flap transfer for soft tissue coverage of the lower leg: the anterior tibial, posterior tibial, and peroneal arteries (FIG 1A-E).
Apart from the concomitant veins of the named arteries of the lower leg, the two major superficial veins, which are the long (great) and short (small) saphenous veins, may be used as recipient veins. The superficial veins run superficial to the fascia cruris (deep fascia) of the lower leg (FIG 1F).
Sizable perforators to the overlying skin derived from any of the three major vessels can also be recipient vessels when they are found near the defect.1,2
The specific recipient vessels are chosen according to the site of the defect.
Upper third of the lower leg: the upper third of the lower leg is technically the most difficult zone for microvascular repairs because of the deep location of major vessels. A long vein graft from the flap passing proximally to the side of the femoral artery was commonly used in the past. However, sural vessels (FIG 2) and the reversed descending branch of the lateral circumflex femoral vessels can also be effective recipient options in this region.3
Middle third of the leg: the anterior tibial vessels are often used because the vessels become more superficial as they descend (FIG 3). The posterior tibial arterial and venous system may be easily exposed after retraction of the soleus muscle when the defect is on the medial side of the leg (FIG 4).
Distal third of the leg: distal branches of all three major vessels are easily accessible in this region because there is less overlying soft tissues, which also makes them more susceptible to injury in traumatic defects. The peroneal artery or its terminating calcaneal artery can also be used in the lateral region of the leg (FIG 5). Perforators from the peroneal artery can be used as recipient vessels in the lateral region (FIG 6).
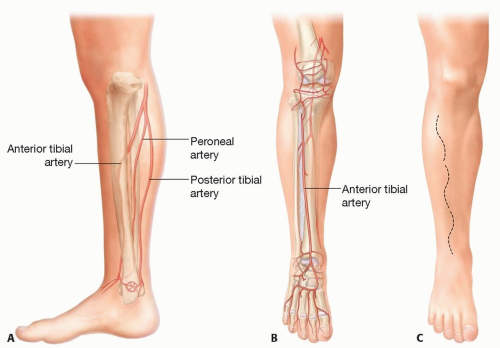 FIG 1 • Main arteries and veins of the lower leg and incisions for exposure of recipient vessels. A. Three named arteries of the lower leg. B. Anterior tibial artery. C. Incisions for exposure of the anterior tibial artery. |
 FIG 1 (Continued) • D. Incisions for exposure of the posterior tibial artery. E. Incisions for exposure of the peroneal artery. F. Long and short saphenous veins. |
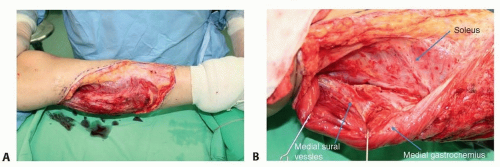 FIG 2 • A,B. Medial sural vessels as recipient vessel. |
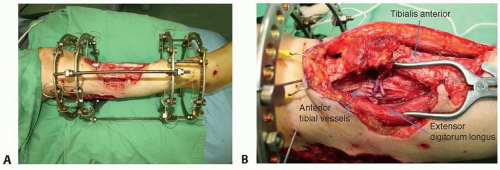 FIG 3 • A,B. Anterior tibial vessels for recipient vessel. |
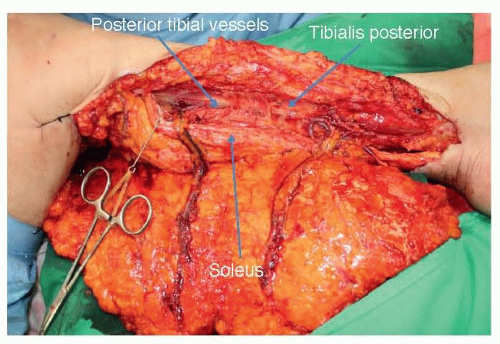 FIG 4 • Posterior tibial vessels for recipient vessel. |
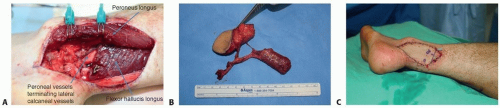 FIG 5 • Peroneal vessels for recipient vessel. A. Peroneal vessels. B. Muscle chimeric TDAP perforator flap. C. After inset of the flap. |
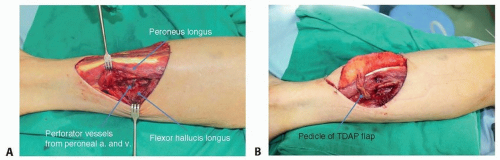 FIG 6 • A,B. Peroneal artery perforators for recipient vessel. |
PATIENT HISTORY AND PHYSICAL FINDINGS
A multidisciplinary approach with comprehensive communication between the oncologist and/or orthopedic surgeon will allow better treatment outcomes.4
Preoperative planning should be carried out by considering anticipated defect size, location, vascular anatomy, and comorbid conditions related to the outcomes of reconstruction.
IMAGING
The authors routinely perform preoperative CT angiography to delineate the vascular anatomy of the lower extremity except when it is contraindicated.
Detailed information of the vascular status helps determine proper reconstruction options and recipient vessels, which ultimately decreases the risk of reconstruction failure in the free flap transfer.5
SURGICAL MANAGEMENT
Soft tissue stability and long-term durability are of paramount concern in the reconstruction of the lower leg.
The simple method is not always the best and often, a more complex method of reconstruction, such as the free flap, is initially chosen to obtain better functional and aesthetic outcomes.
Elaborate preoperative planning regarding recipient vessels, donor site, flap composition (cutaneous, fasciocutaneous, musculocutaneous, chimeric, composite flap), and positioning of the patient during the surgery is crucial for successful soft tissue reconstruction of the lower leg. A muscle chimeric perforator flap is useful for filling dead spaces created by soft tissue loss (see FIG 5).6
Vascular complications are significantly higher if anastomoses are carried out in the zone of injury, due to inflammation and trauma to recipient vessels. A sufficiently longer pedicle or vessel graft may be necessary to reach normal suitable vessels.
Donor site morbidity should also be considered in the preoperative planning. The donor site that permits primary closure of the donor defect is always favored over the ones that require skin grafting. The exact measurement of the shape and size of the defect is valuable for donor tissue economy and acceptable aesthetic results at the recipient site. A customized flap may be effectively designed by using paper or transparent plastic template based on the final defect shape.
The flap thickness can be controlled by defatting of the perforator flap at the time of inset, which facilitates aesthetic reconstruction. On the other hand, flap thickness can be controlled secondarily when tissue edema resolves completely.
Fasciocutaneous flap vs muscle flap in contaminated wounds: A previous animal study demonstrated that muscle flaps have advantages over the fasciocutaneous flap for contaminated wounds.7 However, recent studies show that there is no difference in bacterial eradication and quality of wound healing between muscle and fasciocutaneous flap use.8,9
There is a controversy regarding how early a soft tissue defect should be closed in lower extremity trauma. Early definitive soft tissue coverage may be necessary where vital structures such as blood vessels and peripheral nerves or hardware are exposed.10 The recent advent of negative pressure wound therapy has helped provide additional time for better delineation of nonviable tissues before final reconstruction in large, complex open wounds.11
Preoperative Planning
Vascular anatomy and degree of atherosclerosis are evaluated by preoperative CT angiography (FIG 7).
Donor site and components of the flap are often decided preoperatively according to predicted defect size, location, type of tissue requirement, required pedicle length, surgeon’s expertise, and patient preference.Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Tibial Reconstruction
Tibial Reconstruction
 Reconstruction of Femur
Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


