Olfaction and taste promote satisfaction and protection in daily life. The astute facial plastic surgeon recognizes the importance of a baseline smell test to document the patients’ olfactory status before surgery. After surgery, the surgeon must be alert to the possible mechanisms of hyposmia and anosmia and the pertinent treatment strategies. The surgeon must also understand the importance of counseling the patient and family regarding the cause of the dysfunction and the proper treatments. This article updates the facial plastic surgeon on the importance of smell and taste and associated disorders with a current review of the literature.
The chemosenses of smell and taste contribute to quality of life and environmental appreciation. Not only do these senses guard against toxic and dangerous stimuli, but the ability to smell and taste contributes to the finer qualities of life, including participating in wine tasting, detecting a fresh-brewed steaming cup of coffee, or baking Christmas cookies. Nasal surgery can alter a patient’s olfaction and some patients have unrecognized olfactory loss before surgery. A recent study from Turkey found that practitioners who were educated about olfactory loss were more likely to rate smell loss as important and be more confident in managing smell loss. We advocate that a basic smell test and record of a patient’s olfaction before surgery is key to avoiding both patient injury and legal misfortune. A working knowledge and awareness of the many factors that contribute to a patient’s sense of smell (and taste) is fundamental.
- •
Olfactory testing is crucial for accurately diagnosing chemosensory problems and before nasal surgery as a medical-legal safeguard for a medical practice. There are several easy-to-use smell and taste tests.
- •
Olfaction is a complex process involving both orthonasal and retronasal pathways for olfactory stimulation.
- •
The astute surgeon may identify nasal and systemic disease factors that may play a role in postoperative olfactory loss.
- •
The presence of functioning senses of taste and smell is a major boost to quality of life and safety.
Surgeons must pay attention to surgical risk factors, surgical techniques, and existing preoperative disease because these can lead to olfactory disturbances and permanent smell loss after surgery.
Anatomy
Olfaction
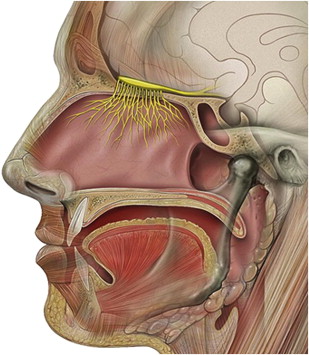
The organs of olfaction are unique within the human body because they contain neuroepithelium that regenerates. However, these delicate nerve fibers may also be damaged and undergo permanent loss. Grossly, the nasal passages contain the structures of olfaction, which include the upper nasal septum, and middle and superior turbinates. These structures facilitate airflow and contain the primary olfactory neurons. Olfactory molecules dissolve in mucous overlying these neurons and then interact with the neurons, producing an action potential. The olfactory bulb, which is positioned at the anterior cranial fossa, serves as the initial transfer station in the olfactory pathway ( Fig. 1 ). The primary olfactory neurons synapse with secondary neurons, which constitutes aggregates referred to as glomeruli. The olfactory cleft lies in a protected location approximately 7 cm from the nasal sill ( Fig. 2 ). Olfactory bulb comes from the Latin words olfactus , which means sense of smell, and bulbus , which means swollen root. This region is where the olfactory nerves (cranial nerve I) terminate and the olfactory tracts arise.