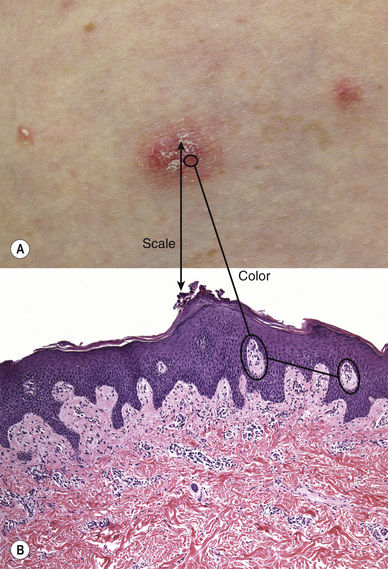
Fig. 5.1Guttate psoriasis. Lesions in (A) developed after a sunburn (Koebner phenomenon).A, Courtesy, Ronald Rapini, MD. A, From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission.
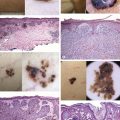
Fig. 5.2Guttate psoriasis. Mounds of parakeratosis, often with neutrophils.
Histopathology:
Slight acanthosis and mounds of parakeratosis that often contain neutrophils (arrow;Fig. 5.2)
Dilated papillary dermal vessels may be present (circles; seeFig. 5.2)
Pityriasis Rosea
Classically starts with a herald patch (often the largest lesion)
• Precedes development of a widespread, symmetric eruption (see below)
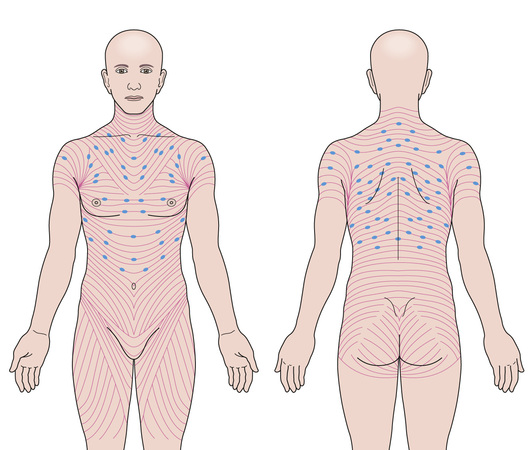
Once well developed, widespread and symmetric (Fig. 5.3)
• Proximal extremities and trunk
• Follow Langer’s lines, forming a “Christmas tree” pattern on the back
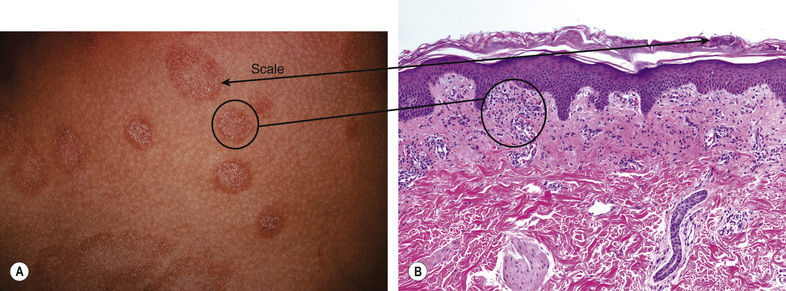
Fine white central scale (arrow) with collarettes overlying round to oval thin salmon-colored (circle) papules/plaques (Figs 5.4,5.5)
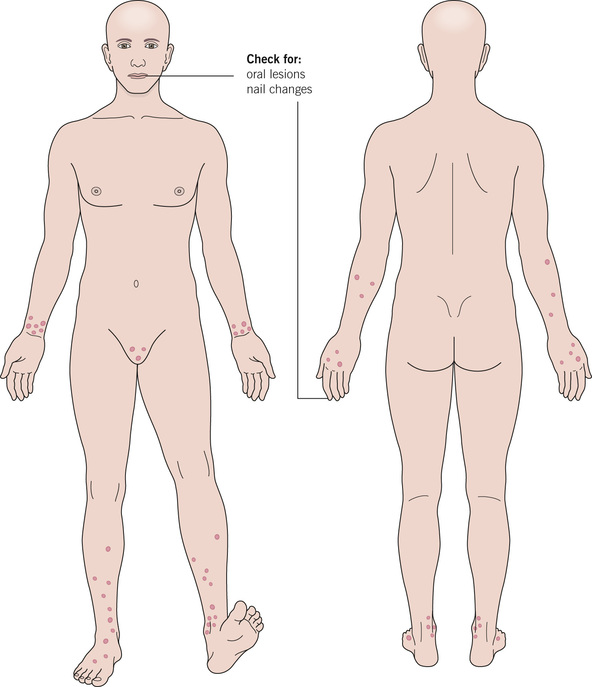
Fig. 5.3Pityriasis rosea. The typical distribution, with lesions oriented with long axes parallel to the red lines (Langer’s lines).From Bolognia JL, Schaffer JV, Duncan KO, Ko CJ. Dermatology Essentials, 1e. Philadelphia: Saunders, 2014, with permission.
Fig. 5.4Pityriasis rosea.From James WD, Berger T, Elston D. Andrews’ Diseases of the Skin, 11e. Edinburgh: Saunders, 2011.
Fig. 5.5Pityriasis rosea.A, Courtesy, Yale Dermatology Residents’ Slide Collection. A,B, From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission.
Histopathology:
Mounds of parakeratosis (arrow; seeFig. 5.5), generally without neutrophils
Fig. 5.8Lichen planus.From Schwarzenberger K, Werchniak AE, Ko C. General Dermatology. London: Saunders, 2009.
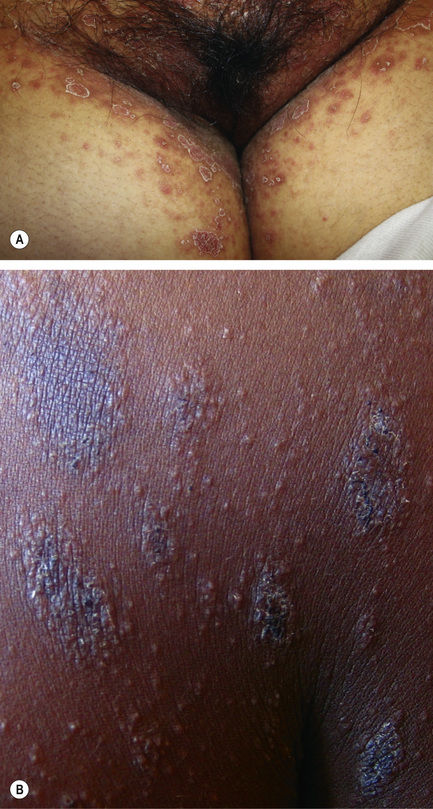
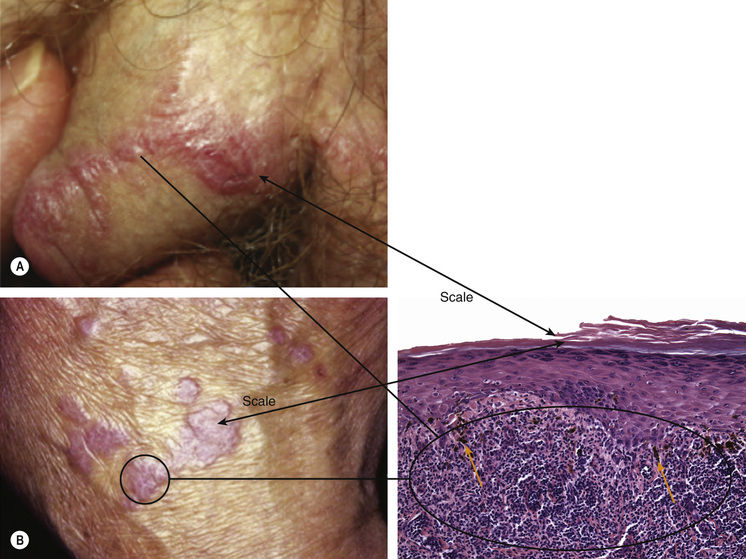
Fig. 5.9Lichen planus. Flat-topped pink to purplish papules with adherent scale. There is hyperkeratosis, hypergranulosis, and lichenoid inflammation.A,B, Courtesy, Yale Dermatology Residents’ Slide Collection.
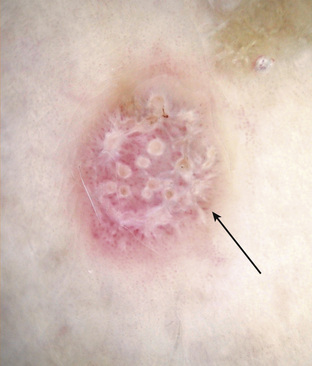
Classic scale is interconnecting white lines (Wickham’s striae) (arrow), possibly corresponding to hyperkeratosis/hypergranulosis (arrow) (Figs 5.9,5.10)
Fig. 5.10Lichen planus, dermoscopy.Courtesy, Iris Zalaudek, MD. From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission.
Only gold members can continue reading. Log In or Register to continue