Skate Flap for Nipple Reconstruction
Katie E. Weichman
DEFINITION
Nipple-areolar reconstruction is the final stage of postmastectomy reconstruction. This procedure has been shown to positively influence overall satisfaction with breasts and outcomes in several series and transforms the mound to a breast.1,2
The skate flap is a commonly performed technique in both implant and autologous reconstruction.
This local flap was first described by J. W. Little in 1994 for nipple reconstruction after mastectomy and breast reconstruction.
Further modifications of this flap have been described by Cordeiro for primary use in implant reconstruction and Hammond for use in autologous reconstruction.3,4
Although there are several additional iterations of the skate flap, the author prefers these two techniques.
The Cordeiro modification to the skate flap has two main advantages.
It avoids elevating the body of the flap with a central wedge of subcutaneous fat as initially described by Little. The central wedge of subcutaneous fat creates a defect that requires primary closure, resultant fat undermining, and significant deformation of the remaining areola. The Cordeiro technique incises through only the epidermis, dermis, and subcutaneous fat without any undermining, resulting in a central subcutaneous stalk for volume without a secondary defect.
A tripoint stitch to the dermal platform is used when the two skate wings are sutured together at the 6 o’clock position.
Hammond’s modification to the skate flap provides the ideal nipple reconstruction for autologous reconstruction. This technique provides a nipple with adequate bulk and long-term projection but uniquely allows for primary closure of the donor site with minimal distortion of the breast.
This technique requires experience with the purse-string technique in breast reduction and mastopexy.
ANATOMY
The skate flap is a local flap with a pedicle of epidermis, dermis, and subcutaneous fat centered at the site of the desired future nipple. The skate flap is named based on skin flaps that are shaped like wings of a skate fish (FIG 1).
Blood supply
Subdermal plexus
Subcutaneous plexus
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients undergoing skate flap nipple reconstruction have reached the end of the reconstructive process.
Indications: A history of breast cancer requiring mastectomy, prophylactic mastectomy, congenital abnormalities, and transgender patients who have had mastectomy with complications associated with silicone injection
History of radiation therapy or need for further radiation therapy should be considered when deciding timing of nipple reconstruction.
Patients should not be actively smoking for at least 3 months prior to surgery.
Patients should have a final breast mound without need for further revision.
Nipple reconstruction should be performed when the breast has taken its final form and has adequately settled to prevent malposition.
This timing is least 3 months to 6 months after either the direct to implant reconstruction, tissue expander exchange for implant, or the autologous reconstruction. All revisions of the breast mounds should be performed prior to nipple reconstruction.
Revision of autologous reconstruction can often be performed synchronously with nipple reconstruction; however, assuring correct nipple position can be more challenging with an increased incidence of nipple malposition requiring further revision.
SURGICAL MANAGEMENT
The authors perform skate flaps for nipple-areolar reconstruction when the nipple-areolar complex is absent.
Patients who desire larger nipples and agree to harvest of full-thickness skin graft from a secondary donor site
(abdomen, inner thigh, or lateral chest wall roll) should be considered for the Cordeiro modification. Patients with autologous reconstruction should be considered for the Hammond modification.
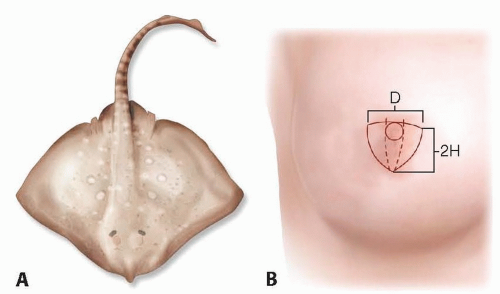
FIG 1 • A. Skate fish. B. Skate flap centered on breast mound. D represents the diameter of nipple and pedicle of nipple; H represents the desired height of the nipple. The length of the flap wings measures at least 3D, and the height of wings measures 2H.
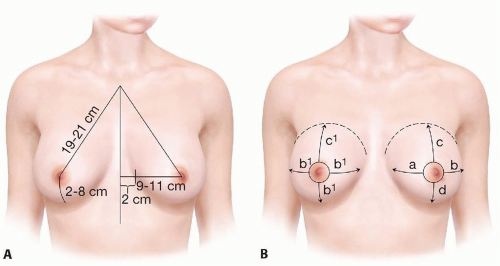
FIG 2 • A. Traditional landmarks for nipple position. Sternal notch to nipple distance of 19 to 21 cm. Distance from midline to nipple measuring 9 to 11 cm. Distance from nipple to inframammary fold measuring 7 to 8 cm. B. Ideal nipple position in asymmetric breasts. Maintain ratios of nipple in relation to the medial breast border, lateral breast border, inframammary fold, and superior breast extent.
Preoperative Planning
Patients are marked in the standing position with shoulders relaxed in the preoperative holding area.
Nipple position should be centered on the breast at the point of maximal convexity and projection. Additionally, it should be symmetric to the contralateral nipple in unilateral reconstructions. In bilateral reconstructions, nipple position is often easier to match, and the location is less critical as long as it is symmetric and located on the center of the breast.
Specific landmarks are often helpful in determining the correct position of the nipple-areolar complex on the breast. These include the level of the contralateral nipple-areolar complex, the position at the Pitanguy point (reflection of the inframammary fold), and triangle from the sternal notch to nipple/midsternal line (FIG 2A).
When breasts are asymmetric, the surgeon should try to maintain the ratios of the nipple to the breast footprint. This includes midline, lateral breast, superior breast, and inframammary fold (FIG 2B).
Positioning
The patient is positioned in supine position. Surgery should be performed in the operating room because a full-thickness skin graft is needed to cover the nipple site.
TECHNIQUES
▪ Cordeiro Modification of the Skate Flap
Flap Design
Generally, the desired diameter of the nipple is designed to be 1 cm. The nipple is marked based on the above guidelines and is confirmed by both the surgeon and the patient as being in an acceptable position.
The use of an EKG lead, as a surrogate for the nippleareolar reconstruction, is routinely used in the preoperative area (TECH FIG 1A).
In unilateral reconstruction, the diameter of the areolar is matched to the contralateral breasts and is generally 38, 42, or 48 mm. A cookie cutter template is used to create a perfect circle (TECH FIG 1B).
In bilateral reconstruction, choice between 38 and 42 mm is made by the surgeon and patient, and the cookie cutter template is used to create a perfect circle.
The axis of the skate flap is designed so that the mastectomy scar does not cross either the wings or body of the flap.
A horizontal line is then drawn cephalad or cranial to the desired nipple location depending on the mastectomy scar to form a hemicircle that will be de-epithelialized and the opposite hemicircle that will be used to construct the skate flap.
Based on this, the nipple reconstruction will be superiorly or inferiorly oriented based on the mastectomy scar (TECH FIG 1C,D).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree