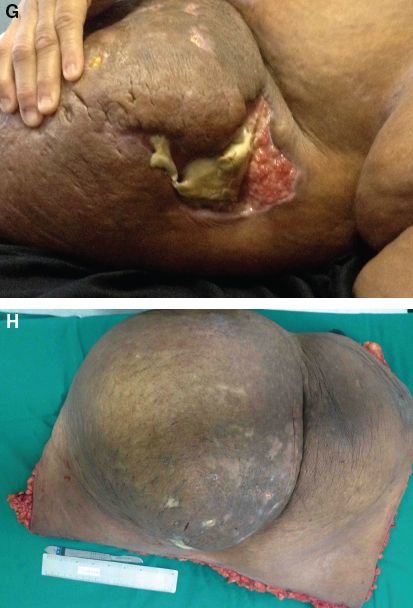
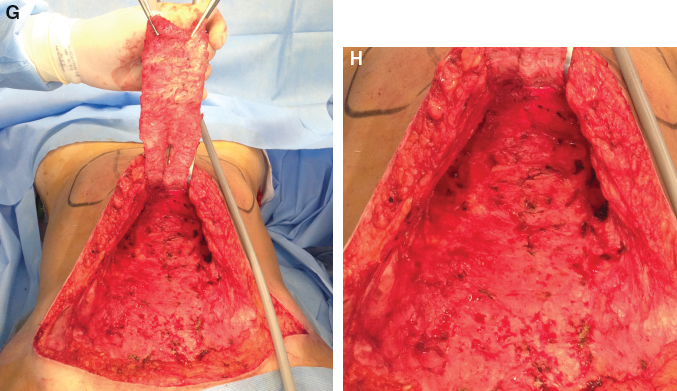
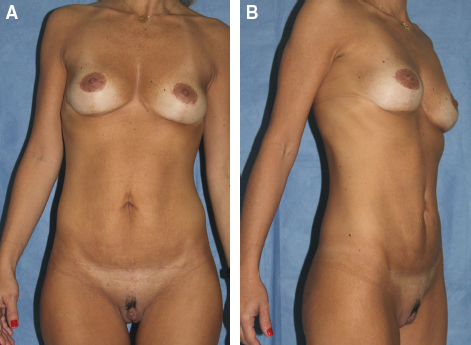
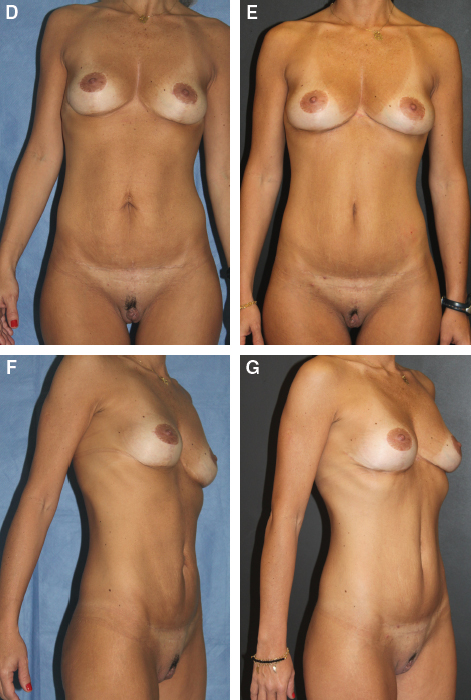
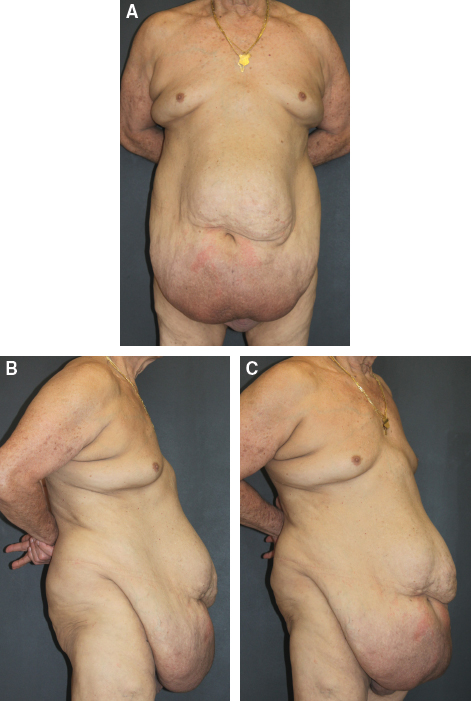
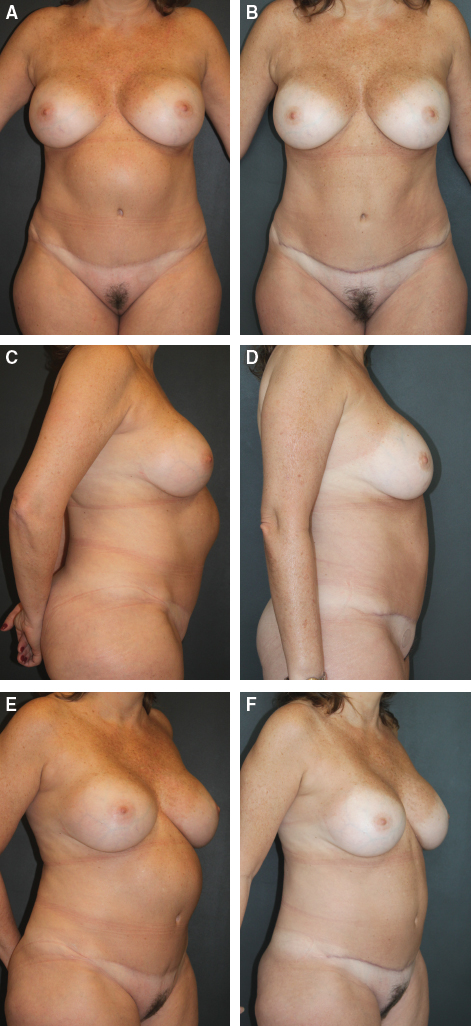
CHAPTER 9 Fig. 9-1, A and B This 40-year-old woman had undergone a mini-abdominoplasty 2 years earlier. She also had a previous mammaplasty. She complained of a supraumbilical excess of skin and a horizontally shaped umbilicus. We designed a reverse abdominoplasty using the previous mammaplasty scars, extending in the midline and liposuction of the flanks. The reverse abdominoplasty was performed, anchoring the flap in the aponeurosis using quilting sutures. This is the final aspect of the incision of the reverse abdominoplasty. The incision is coincident with the submammary fold, where two previous mammaplasty scars were located. Fig. 9-1, D-G The patient is seen before and 8 months after surgery. Note the improvement of her umbilical shape and abdominal contour, and the acceptable lateral extension of the submammary scar. Fig. 9-2, A-C This 58-year-old man presented with a BMI of 40 and a history of chronic alcoholism with cirrhosis. He had a platelet count of 60,000; his pannus had lymphedema, fibrosis, and a chronic infection in the infraumbilical area. He also had a groin hernia that required reconstruction with mesh. The patient was treated with intravenous antibiotics, but the infection recurred soon after the course of antibiotics was completed. Gastroplasty was contraindicated by the bariatric surgeon. His surgeries were planned as two procedures. In the first, the redundant skin with the site of infection was removed. The patient had an uneventful outcome. Six months later, a fleur-de-lis abdominoplasty was performed, and the groin hernia was corrected using mesh. His final result is shown at 8 months postoperatively. A total of 8 kg of fat and skin was removed. Before the second procedure, the patient’s weight was 96 kg and as seen in the final result, his weight was also 96 kg. (The patient gained 8 kg during the entire treatment process.) Fig. 9-3, A and B This 43-year-old woman with a BMI of 56.3 presented with psoriasis and extensive lymphedema of the pannus. The bariatric surgeon had indicated 2 years before that gastroplasty was contraindicated in this patient. However, she developed a severe infection of the pannus, with areas of necrosis and sepsis. She was sent to the ICU, where she was treated with antibiotics, and the plastic surgery team was consulted. We planned an abdominal wall amputation with removal of the infected site. We removed 15 kg of fat and skin from the lower abdomen. Some infraumbilical skin was left in the midline to keep the umbilicus in the anterior abdominal wall, although it cannot be seen in the postoperative frontal view because of the heavy supraumbilical fat excess. Three days after the operation, the patient was discharged from the hospital and given oral antibiotics. She healed well, with no recurrence of the pannus infection. The patient is shown before and 2 years after surgery showing the removal of the infected site by abdominal amputation. The umbilicus was retained in the lower part of the abdomen to be reinserted in a higher position in the abdomen. No umbilical transposition was made at this time to avoid contamination from the infected site. Note the areas of necrosis at the lower aspect of the abdominal fold. The skin and fat removed had intense fibrosis and necrotic areas and weighed 15 kg. Fig. 9-4 This 46-year-old woman had undergone an abdominoplasty 2 years earlier. She presented with a projection of the upper abdomen that had begun to develop 3 months after surgery; she reported that the deformity had increased in the months that followed. Ultrasonography showed no recurrence of rectus diastasis; some fibrosis was detected in the area. The deformity was diagnosed as a pseudobursa. The plan for this patient was to remove the pseudobursa and use quilting sutures to attach the flap to the fascia. A very thick capsule was found and removed. Quilting sutures were placed every 2 cm. She is shown 8 months after the secondary abdominoplasty showing correction of the projection that had been caused by the pseudobursa. Fig. 9-5, A-F This 52-year-old woman had abdominoplasty 2 years earlier with placement of a mesh in the area of the supraumbilical diastasis. She reported that 2 months after the operation, a bulge began to develop in the supraumbilical area that increased over the following months. An MRI demonstrated recurrence of the rectus diastasis only at the supraumbilical area. We planned a surgery to correct the rectus diastasis by advancing the recti sheaths, as in a type C deformity.
Secondary and Atypical Cases in Abdominoplasty
Case 1
Case 2
Case 3

Case 4
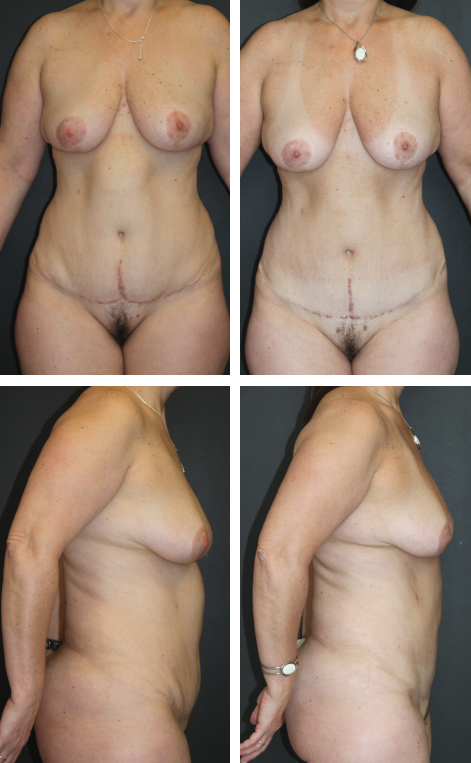
Case 5
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine