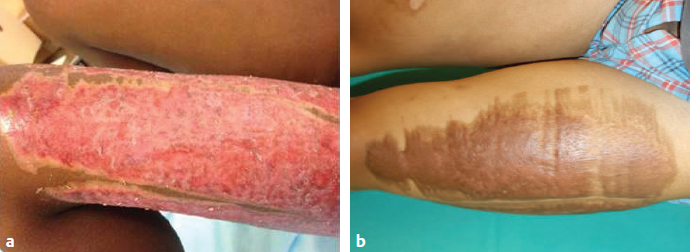
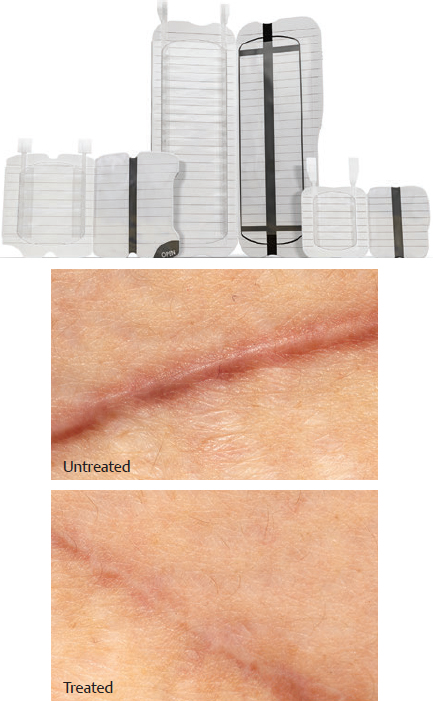
CHAPTER Patients regularly come to a plastic surgeon because they are unhappy with a scar. Many times this means that their tissues have responded to an injury or surgery with a healing result that has not restored the skin to normal. Often the tissue response results in little scarring but rather exhibits abnormal contour or pigmentation. It is possible to treat these problems, but not with the same techniques as used for exaggerated scars. Although wounds always heal with some scarring, excessive scarring disturbs patients by limiting functional and aesthetic outcomes. A surgeon with a mechanistic knowledge of how wounds heal can limit these complications. However, perfect healing seldom occurs. Correction of scar deformities requires thoughtful application of the breadth of reconstructive techniques. Even the most precise surgeon will sometimes have patients who have unsightly postoperative scars. Understanding how to manage the consequences of dysregulated healing and exaggerated scar requires an understanding of cutaneous wound healing. Very superficial epithelial skin injuries regenerate normal anatomy. Deeper injuries, including surgical incisions, do not regenerate normal structure but rather scar. The difference is in how much scarring occurs. The restoration of dermal continuity achieved by suturing cut dermal edges occurs when disorganized collagen fibers cross-link to the organized dermis that formed during development. Recognizing the external influences on this scar and managing them is an essential component of scar treatment. Understanding how wound healing occurs is also essential to managing the final result. Wound healing is a highly organized, interrelated set of biochemical and cellular responses. These events need to proceed in a specific manner for the wound to heal optimally. Release of platelet-derived growth factor (PDGF) and transforming growth factor beta (TGF-β) from platelets during hemostasis induces an inflammatory recruitment that includes the macrophages, which then orchestrate the matrix synthesis that becomes scar. Restoration of the epithelial barrier decreases the inflammatory signals, matrix synthesis, and scarring. Ongoing or persistent inflammation stimulates continued production of the mediators, which induce matrix protein synthesis. Wound remodeling occurs in response to mechanical signals in the wound. Newly synthesized matrix contracts as cells that were required for wound healing migrate out of the wound. After attachment to newly synthesized and uncross-linked collagen, they activate myosin and actin, pulling together the protein fibers. During optimal healing, matrix synthesis wanes in a few weeks. Remodeling continues for months. When wound healing becomes abnormal, the result is either failed healing or excessive scar. Ongoing hemorrhage or blood within the tissues induces ongoing inflammation, resulting in scar contusions and nonhealing, as occurs during the venous hypertension of venous disease. There is also usually significant scar in such tissues. If the wound inflammation does not wane, matrix synthesis continues, and increased scar forms. This happens when wounds are infected or are closed poorly or if the patient has an intrinsic or extrinsic wound-healing abnormality that delays healing. Many of these situations are under the control of the surgeon (Figs. 12.1 and 12.2, Box 12.1). Fig. 12.1 Deep second-degree burn of the medial thigh. Healing without grafting will predictably result in a hypertrophic scar. Grafting the thigh will improve the scar but will create a donor site scar. Preventable • Wound infection • Poor nutrition • Tissue tension • Technical failure Unpreventable • Preexisting healing derangement • Patient age • Comorbidities that affect healing: Fig. 12.2 (a) A skin graft donor site that healed poorly after 8 weeks because of patient scratching, poor nutrition, and inadequate wound care. (b) The hypertrophic scar 1 year later, currently under treatment with compression and silicone. Fig. 12.3 Twelve months after a second-degree burn of the chest and upper arms that healed uneventfully. Significant scarring is present at areas of stretch in the sternum and shoulders. In addition to the biochemical events already discussed, tension increases scar spreading and hypertrophy. Sites like the sternum, where the skin is fixed and motion increases tension, are well-recognized examples of this (Fig. 12.3). The implication of these facts is that some scar is normal, but excessive scar is not. Robson1 described abnormal scarring as proliferative, because unfavorable scars are usually the result of exaggerated scar formation. In addition, scars can be of normal thickness but have spread or widened. I describe these as normal scar, spread scar, or hypertrophic scar.2 There is also a pathologic exaggerated healing response, called a keloid. There is much misunderstanding about the distinction between a keloid and a hypertrophic scar. They are not the same disease. They have different pathophysiologic mechanisms.3 A hypertrophic scar is exaggerated normal healing, usually the result of large injuries that heal slowly. The classic cause for hypertrophic scarring is a burn injury, in which delayed wound closure and prolonged inflammation often result in hypertrophic scarring. Hypertrophic scars get worse for 3 to 6 months, then improve for 12 to 24 months. Patients with a hypertrophic scar heal normally before and after the event that triggers the scar (Fig. 12.4). Fig. 12.4 Minimal shearing around this skin graft resulted in several millimeters of ungrafted full-thickness wound. This healed slowly. The surrounding “frame” of hypertrophic scar is the area that was not successfully grafted and healed poorly. When healing exceeds the restorative needs of tissue integrity, it should be considered excessive. The two types of excessive (proliferative) scar are hypertrophic and keloid. Most experienced clinicians and scar researchers consider these two distinct entities. They have different clinical expressions, cell biology and biochemistry, and response to treatment. Although there have been hundreds of scientific studies on the pathogenesis of abnormal scarring, neither type is fully characterized. The global summary of this research is that changes in cell function, matrix composition and organization, and tissue microenvironment all occur.4 Most investigators believe that hypertrophic scar is an exaggerated version of normal wound-healing mechanisms and keloid is a distinct physiologic response. There is general agreement that hypertrophic scarring occurs after excessive inflammatory states, likely mediated by dysregulated T helper 2 responses. The result is excess local TGF-β and thus an increase in matrix synthesis and contraction5,6: exaggerated participation by bone marrow–derived mesenchymal cells, particularly fibrocytes, keratinocyte, and endothelial hyperproliferation; and abnormal protease regulation.7 The most common contributor to this process is delayed healing, as often occurs in serious burn injuries. Keloid pathophysiology is even less well understood. Some researchers believe that TGF-β is also involved in keloid pathogenesis, and that keloid fibroblasts are genetically abnormal in their responses to stimulatory factors compared with their hypertrophic and normal scar counterparts.8 This suggests that keloid proliferation originates from one genetic mutation and that the keloid fibroblasts should be monoclonal. However, clinical experiments show that keloid fibroblasts are polyclonal in nature.9 Attempts to classify keloid histopathology have also led to conflicting reports, with some describing an absence of dermal nodules in keloids, whereas others have determined that these dermal nodules are present, though less well defined in keloids as opposed to hypertrophic scars.3,10 Still others believe that scars have a dynamic morphology and differences in characterization are a result of incomplete sampling.11 These data may result from the asymmetrical nature of keloid scars, which tend to have more quiescent centers and more active peripheral edges. Collagen imbalance is another dysregulated pathway that has been studied. In normal scars, collagen 1 and 3 increase with time, but the proportion of collagen 3 decreases as scars mature. In hypertrophic scars and keloids, the relative amount of collagen 3 remains increased even in scars that have been present for up to 20 years.12 Summary Box Complications Associated with Scar Revision Excessive scarring: Hypertrophic scar Keloid scar Delayed healing because of infection The best way to treat a problem is to prevent it. Preventing scarring involves closing wounds as early as possible and with no tension. I achieve these goals with a staged strategy. Elective surgical incisions should be closed with precision, usually in layers. When there is tension, I use a buried polyglyconate or polydioxanone suture to anchor the dermal edges together during the initial several months of wound healing. Other absorbable sutures and removable sutures lose this ability after a few weeks, resulting in scar spreading and hypertrophy. Acute skin trauma cannot be treated this way because of the general tissue damage and presence of bacteria. A common cause for delayed healing is infection. A topical antimicrobial is an easy and effective adjunct to wound closure and can limit this problem. For simple incisions and wounds I use 2% mupirocin, because it is highly effective against Staphylococcus and Streptococcus spp., the usual agents of infection. For larger wounds or burns, skin grafts, and donor sites, the broad-spectrum benefits make silver sulfadiazine or a silver-releasing dressing ideal choices. In my practice all wounds are treated with an antimicrobial dressing. Fig. 12.5 A distal foreleg that has been grafted with Integra dermal template. The Integra was lost in the area noted. The entire leg was regrafted with thin meshed autograft. The appearance of the area with successful Integra engraftment is improved. Fig. 12.6 This patient demonstrates many of the deformities of an untreated scar: scar contraction on the flexor surfaces of the digits and the extensor surface of the dorsum, hypertrophic scar at the shear planes between grafted and ungrafted skin (note the ulnar side of the thumb), hypertrophic meshed patterning at the forearm, and linear scar bands at proximal wrist where dorsiflexion occurs. These would have been significantly more normal in function and appearance with monitored use of silicone and pressure garments. Fig. 12.7 Embrace device used to minimize scar hypertrophy and spreading. (These images are provided courtesy of Neodyne Biosciences, Inc.) An important consideration is that successfully closing larger wounds has other priorities than creating the best scar. In many cases the plastic surgeon must develop a plan with the patient that balances faster, more simple wound closure and best long-term results. An example of this conflict is the choice of meshed versus sheet grafts. A more sophisticated example is the decision of whether to use Integra regenerative dermal template (Integra LifeSciences) to improve the appearance of widely meshed skin grafts (Fig. 12.5). By providing a template for dermal regeneration, the product creates a thicker graft with the predictable improvement in appearance. This improved appearance does come with increased cost, however. Finally, although some large wounds might heal over a period of 4 to 6 weeks, the resulting scar will be significant. Patients and physicians need to discuss whether limiting scarring with a graft, adding a modest donor site scar, is a better strategy for improved appearance. Wounds that are closed incompletely often form hypertrophic scars. This includes imprecisely closed incisions that heal over days rather than hours. Incompletely grafted wounds or widely meshed donor sites similarly heal with more scarring and often become hypertrophic (Fig 12.6). Scars spread when the mechanical forces on the uncross-linked matrix are sufficient to pull matrix fibers apart. Avoiding excessive tension prevents this. The benefits of deep buried sutures were mentioned previously. Reorientation of tension with z-plasties or other local tissue rearrangements also helps. There are many strategies to decrease tension with taping, external appliances, and massage. The best method to prevent scar spreading and the only one of proven effectiveness is the Embrace device (Neodyne Biosciences; Fig. 12.7). This is externally applied up to 2 weeks after surgery to a closed, dry incision and limits tension being transmitted to the uncross-linked, newly synthesized matrix of the incision. Strategies that cause the wound to heal quickly are the best tools for prevention of unattractive healing. Prevention of infection, stretch, and shear were discussed previously. The most common cause for unsightly healing in my practice is hyperpigmentation. Wound healing activates melanocytes, which make more melanin in response to ultraviolet light. The result is noticeable and disturbing. Hyperpigmentation is most noticeable in patients with Fitzpatrick type 3 or 4 skin color but can result in a noticeable difference in anyone except patients with the lightest or darkest skin color. Prevention with sunscreen is the best treatment, although tretinoin and quinolones are effective when hyperpigmentation develops. I ask patients to routinely use sunscreen with a sun protective factor of 30 or greater until the wound is not red. Although most plastic surgeons practice nonoperative scar management, there is little objective data about the various treatment options. (There is data about the treatment of keloids, which are discussed later.) Most surgeons are very willing to attribute scar improvement to their treatment algorithms. However, the natural history of normal and hypertrophic scars is to spontaneously improve 3 to 12 months after injury. I use available treatments but try to be realistic. There are three accepted ways to nonoperatively treat scars (Fig. 12.8): 1. External pressure 2. Silicone sheeting 3. Pharmacologic treatment with steroids Pressure garments have been shown to produce scars that are thinner, softer, and lighter in color than scars from the same injury that healed without pressure garments at up to 1 year of follow-up.13 For these external pressure modalities to work, they must be monitored and adjusted at regular intervals. Although the scars may remain thick, the pressure garments typically cause flattening of contour irregularities. If not, they should be adjusted. Silicone sheeting can be used to line pressure garments or used alone. When used alone, silicone sheeting can be applied for only 12 hours a day.14 This treatment increases patient compliance, because the scars can be treated at home, outside the workplace. Scars show improvement after treatment for 2 to 3 months without further follow-up.15 Corticosteroid injections are one of the oldest and most accepted treatments for abnormal scarring, with the greatest and most lasting benefit occurring in those who receive the injection earlier in the scar healing process16 (Fig. 12.9). There is general agreement that triamcinolone injections induce short- to long-term improvement in both keloids and hypertrophic scars (Table 12.1). Steroid treatments for abnormal scars have not been completely investigated at more long-term follow-up periods, but keloids have been known to recur more than a year after initial treatment. This means that despite being universally used, corticosteroid injections provide an unproven long-term benefit. In my experience, they improve symptoms of pain and itch in keloids but provide only temporary benefit to keloid scar mass.
12
Scars and Scar Revisions
Excessive (Proliferative) Scar
Hypertrophic Scar and Keloid Scar
Wound Healing

 Diabetes
Diabetes
 Cancer
Cancer


The Science of Scarring
Avoiding Unfavorable Results and Complications in Scar Revision Surgery
Preventing Scarring


Limiting Unsightly Healing
Managing Unfavorable Results and Complications in Scar Revision Surgery
Treating Scarring
External Pressure
Silicone Sheeting
Steroid Treatment
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine










