Scar Revision and Local Flap Refinement
Scar Revision
Wound Healing and Contributing Factors
Factors that influence scar formation and appearance after wound healing depend on the initial injury, location of the wound, and local cellular and humoral responses.1–3 Wound healing is a natural phenomenon that progresses through many states before complete healing. The stages of wound healing include initial coagulation, inflammatory phase with re-epithelialization, fibroblastic phase, and maturation phase with the deposition of collagen and glycoproteins.2 The process of healing is complete after approximately 1 year, at which time the scar will reach 80% of the original tissue tensile strength.4 Wound healing is discussed in detail in Chapter 4.
The circumstance of wounding is a factor in scar formation. Planned surgical wounds heal better than contaminated wounds.5 Skin wounds from traumatic injuries or disease usually heal with more scarring. In traumatic and surgically created wounds, greater tissue loss is associated with greater scarring. When lacerations or skin avulsions are ragged but parallel to relaxed skin tension lines (RSTLs), the irregular borders can be excised and the wound closed in a straight line. However, if the wound is perpendicular to RSTLs, it may be prudent to close the wound while preserving the ragged border to help create an irregular scar.6 Thermal injuries and wounds containing foreign material are likely to heal with hypertrophy.3
Optimizing a patient’s nutrition and immune system is beneficial to wound healing. Collagen synthesis requires vitamins A and C and iron. Epithelialization requires zinc. Certain chronic diseases affect wound healing. Patients requiring insulin for diabetes, steroids for collagen vascular disease, or antimetabolites for cancer have an increased risk of poor wound healing and wound infection.7 Individuals with atrophic dermatitis or psoriasis tend to have staphylococcal colonization of their skin and as a consequence have a higher risk of postoperative wound infections. Wounds created in areas previously treated with 50 Gy or greater of irradiation are more likely to heal slowly or not at all. This is due to irradiation-induced changes of the skin that include fibrosis and obliteration of the subdermal vasculature, atrophy of the skin and subcutaneous fat, and loss of cutaneous appendages.7 Nicotine can increase the risk of skin necrosis after wounding. This is due to the effects of nicotine on the vasculature of the skin, which include endothelial thickening and damage to small vessels. It is also related to the vasoconstrictive properties of nicotine.
Ideal Scar
To achieve an ideal scar when performing flap surgery, the surgeon must have a thorough understanding of skin anatomy and physiology, perform careful analysis of the defect, be knowledgeable concerning alternative reconstruction methods, employ skillful and meticulous soft tissue handling techniques, and understand the patient’s expectations. The surgeon must also be aware of the limitations of each surgical procedure. When alternatives are available, the surgeon should avoid creating long, straight, unbroken incisions that tend to make scars more visible.8,9
Timing of Scar Revision
Traditional teaching dictates that scar revisions should not be performed until 6 to 12 months after the initial surgery or wounding. This is to allow scar maturation. Wounds have only 20% of their final strength by the third week of wound healing.10 Scars continue to change and to improve during the remodeling phase of wound healing. This includes collagen remodeling and collagen fiber reorientation for up to 18 months. This process can be longer in children. Young patients may have an exaggerated healing reaction with increased scar erythema and hypertrophy, so scar revisions in children should be delayed as long as feasible (Fig. 27-1). Immature scars tend to be erythematous, which will usually fade over time (Fig. 27-2). The scar’s appearance will also improve as it matures. However, early scar revision may be necessary if scars are grossly deforming, such as those that are perpendicular to RSTLs, cross or deform facial aesthetic regions or units, or have traumatically implanted foreign material. In such circumstances, it is recommended to delay scar revision for only 2 or 3 months after wounding to allow the deposition of dermal scar, which can serve as a wound base. Dermabrasion of scars may be performed 6 to 9 weeks after initial wounding. The first 2 months of wound healing manifest a high fibroblast activity and collagen remodeling; therefore, dermabrasion is more effective at this time.11,12
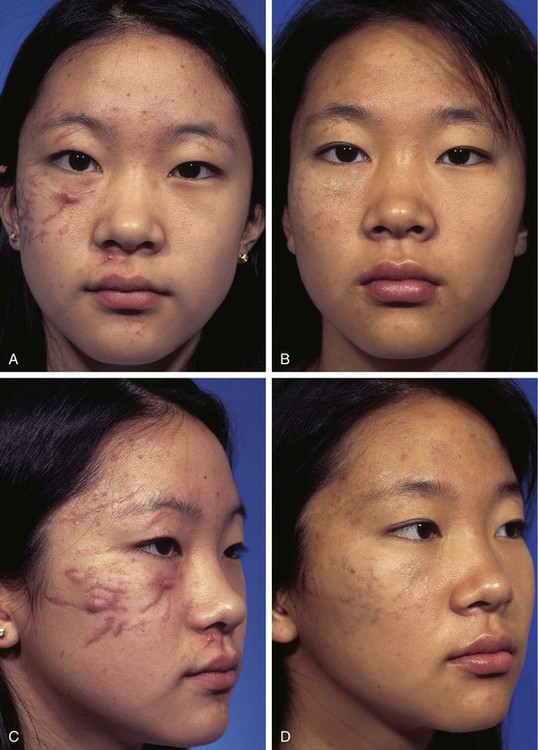
FIGURE 27-1 Multiple facial scars in a 13-year-old patient after an automobile accident. A-D, A few weeks after the accident and 3 years later. Scars matured and erythema regressed. Scars were treated with single intrascar injection of triamcinolone in select areas and silicone sheeting over all scars at bedtime for 1 year.

Patient Assessment
An understanding of the mechanical properties of facial skin and the principles of facial aesthetic regions and units is necessary to perform skillful scar revision surgery. Skin anatomy is discussed in depth in Chapter 1. Facial aesthetic regions and units are described in Chapter 6. A history of how the patient has healed from previous injuries is important. Patients who can bend their thumb back to the volar surface of their forearm (Fig. 27-3) or touch their tongues to their noses (Gorlin’s sign) are more flexible than the average person. These individuals possess more elastin within their dermis and are more likely to spread their scars.


FIGURE 27-3 A, Patients who can bend thumb back to volar surface of forearm possess more than average elastin in dermis. B, Same patient showing facial scars from varicella. Increased elastin in skin causes scars of all types to spread as they mature.
Patients should discontinue the use of tobacco products, nonsteroidal medications, and vitamin E before scar revision. Scar revision should not be performed in an area of active infection. Active acne should be controlled with antibiotics, topical retinoic acid, and keratolytics.7 If the patient has been taking isotretinoin (Accutane) within 18 months, dermabrasion or laser resurfacing should be postponed. Isotretinoin reduces the cellular activity of cutaneous adnexal appendages that is necessary for re-epithelialization of superficial surface wounds. Before dermabrasion or laser resurfacing, the skin may be conditioned by treatment with a tretinoin. Tretinoin has been shown to inhibit dermal collagenase, preventing breakdown of collagen. Patients should be instructed to avoid excessive sunlight exposure to a scar before and for 3 months after revision surgery.
Techniques
Scar Excision
Excisional techniques are designed to reduce wound closure tension, to change the shape of a scar, to correct uneven tissue apposition, or to fill in contour depressions. The most common excisional technique is the elliptical excision, which is used for scars that are elevated or depressed in relationship to the level of the adjacent skin. Elliptical excision is also useful for treatment of malaligned or wide scars and those that can be repositioned into an aesthetic boundary. Elliptical excision is often reserved for scars that are parallel to RSTLs or in favorable areas of the face and less than 2 cm in length. Elliptical excision is particularly useful for individual ice pick acne or pox scars or short, straight, wide, depressed, or raised scars. Fusiform incisions are made parallel to RSTLs or in aesthetic boundaries. The ellipse is designed with angles of 30° or less at each end to prevent skin redundancy. To shorten the elliptical excision, an M-plasty may be performed. Excisions that are longer than 1 cm may be designed sinusoidally and parallel to contour lines or RSTLs. Compared with a standard elliptical excision, a lazy S–shaped excision may close easier and avoid bunching at the ends of the wound with less midpoint wound closure tension.13 The length-to-width ratio of elliptical excisions should be 3 : 1 to allow wound closure without standing cutaneous deformities. If standing cutaneous deformities form, they can often be corrected by sewing out the extra length. When the two borders of an incision are unequal in length, a standing cutaneous deformity may occur along the border of the wound with the longest length. An equalizing Burow triangle can be excised to shorten the long border. This consists of making an incision perpendicular to the long side of the wound and removing a triangle of skin. In performing an elliptically shaped scar excision, it is helpful to leave the deeper dermal scar in situ to augment the depth of the wound. Most scars are excised just outside of the scar margins; however, keloids and hypertrophic scars heal with less hypertrophy if they are excised slightly inside the margin of the scar.14,15
Scar excisions in the form of skin punch excisions to treat ice pick–type acne scars may be beneficial. The depressed scar is punched out with a skin punch and discarded. The edges of the wound are approximated with eversion. This works well if the adjacent skin is normal. Punch grafts from the postauricular skin can be placed into the hole created by excised ice pick scars. Punch excisions and grafts are usually followed by dermabrasion within 6 weeks to achieve optimal results.16 Punch incision can also be performed and the scar plug elevated and sutured to the adjacent skin.
Partial or multiple serial excisions of scars may be used when the elasticity of the scar and surrounding tissue prohibits one-stage excision. Stress-relaxation causes tissue to stretch over time, which facilitates re-excision of scars.17 Serial excision is a particularly useful technique for removal of skin grafts or pigmented lesions (Fig. 27-4). It may also be an effective method for excision of broad scars and burn scars or where severe disfigurement would occur if the area were excised in one stage. Tissue expansion can accomplish the same goal as serial excisions of scars but in two or more stages. Tissue expansion uses the advantage of the stress-strain curve beyond the elastic limit of skin.18 Adjacent tissue usually provides the best skin color and textural match for repair of wounds. Thus, tissue expansion or serial excision provides a method of transferring like tissue into an area deficient of skin where a single surgical stage does not provide a means to accomplish this.18
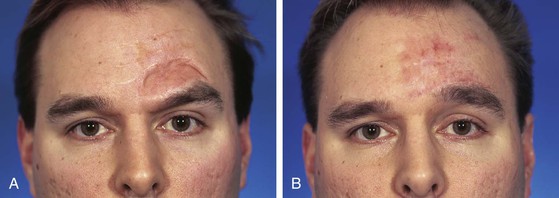
FIGURE 27-4 A, Full-thickness skin graft of left side of forehead. B, One year after serial excision of graft.
Proper tissue handling is important for successful scar excision techniques. Undermining in the subcutaneous tissue plane at least 1 cm beyond the borders of the scar excision is necessary to reduce wound closure tension.17 Dermal approximation is recommended to reduce tension and to eliminate dead space. Accurate alignment of muscles is necessary for proper restoration of function. Absorbable sutures are used for dermal apposition with attention toward precise eversion of wound edges to prevent discrepancies in the level of the epidermis. Eversion of the skin edges of a wound can be accomplished with deep subcutaneous sutures, epidermal vertical mattress sutures, or simple cutaneous sutures placed perpendicular to the skin surface. Unequal depths of the bites of the dermis on either side of the wound may be necessary to create a level everted wound edge. There is much controversy concerning the preferred method and materials used for closure of wounds. Issues include the use of absorbable or nonabsorbable cutaneous sutures and whether to repair a skin incision with simple running or mattress sutures. Karounis et al19 and Singer et al20 studied the issue of absorbable versus nonabsorbable cutaneous sutures and found that the repair of traumatic lacerations in children with absorbable sutures appeared to be as acceptable as that with nonabsorbable sutures. The long-term aesthetic results were deemed to be similar.19,20 An in-depth discussion of wound closure techniques is presented in Chapter 4.
Scar Irregularization
Z-Plasty
Z-plasty is a form of scar irregularization. It can be used to interrupt scar linearity, to elongate contracted scars, to efface webs or clefts, and to change the orientation of scars so that the majority of the length of a scar is aligned with RSTLs.9,17 Z-plasty can also be used to correct distorted anatomic facial landmarks caused by scars (Figs. 27-5 and 27-6). An example of this is use of a Z-plasty to lengthen a scar causing lower eyelid retraction.21 Z-plasty can realign a scar that crosses the alar-facial sulcus or melolabial crease. Z-plasty is an effective method of reducing trap-door deformity.
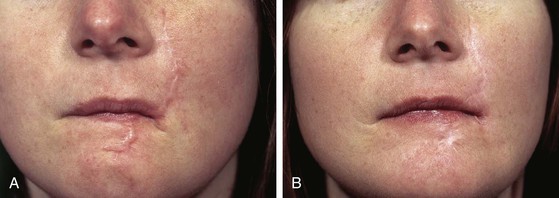
FIGURE 27-5 A, Hypertrophic scars of cheek and upper and lower lips after a dog bite. B, Improvement of scars after staged Z-plasty procedures (three stages) and dermabrasion.

FIGURE 27-6 A, Scarring of upper lip with distortion of vermilion border. B, After multiple Z-plasties and two dermabrasions of scars.
In designing a Z-plasty, all limbs and angles of each triangular flap are equal to each other. The angles of the tip of the flaps may vary from 30° to 60°. The degree of release of contracted scars by Z-plasty is related to the size and angulation of the triangular flaps of the Z-plasty. Flaps of 60°, 45°, and 30° will have the effect of releasing a contracted scar by approximately 75%, 50%, and 25% and changing the orientation of the scar 90°, 60°, and 45°, respectively.2 The final position of the new central limb of the Z can be predicted by envisioning an imaginary line that connects the two free ends of the original Z.
Z-plasty is a powerful and effective method of correcting distortion of the vermilion or realigning irregularities of the vermilion. Figure 27-7 shows distortion of the vermilion after an A-T wound closure of a 1.5-cm skin and vermilion defect of the upper lip. The deformity was first corrected by employing a double Z-plasty to lower the level of the vermilion border in the midline (Fig. 27-7E). A second surgical stage was performed to reconstruct a Cupid’s bow. This was accomplished by using a V-Y island advancement flap based on a subdermal orbicularis muscle pedicle. A small ellipse of vermilion was excised to create a midline tissue void that allowed inferior advancement of the island flap to create the resemblance of a Cupid’s bow (Fig. 27-8). This is an effective method of restoring this important landmark of the upper lip. Another example of this technique is discussed in Chapter 9.

FIGURE 27-7 A, A 1.5 × 1.5-cm defect of skin and vermilion repaired with A-T wound closure (see Chapter 9). B, Scar contraction caused distortion of vermilion. C, D, Double Z-plasty used to correct distortion. E, Postoperative result at 3 months.

FIGURE 27-8 A, Same patient shown in Figure 27-7. V-Y island advancement flap based on orbicularis oris muscle pedicle designed to restore Cupid’s bow. Flap advanced inferiorly after resection of small ellipse of vermilion. B, Flap in place. C, Postoperative result at 1.5 years. Resemblance of Cupid’s bow restored to vermilion border.
Figure 22-9 shows distortion of the vermilion border of the upper lip after reconstruction of a 2 × 2-cm skin defect with a rotation lip flap. The distortion resulted from contraction of the vertical scar along the length of the medial border of the flap. In addition to causing distortion of the vermilion border, the scar was excessively wide and exhibited a slight depressed contour. To correct the vermilion deformity and to improve the contour of the scar, a Z-plasty was performed. This was successful in restoring a natural border to the vermilion and in correcting the depressed scar.






FIGURE 27-9 A, A 2 × 2-cm skin defect of upper lip. Rotation flap designed for repair. Anticipated standing cutaneous deformity (horizontal lines) marked for excision. Z-plasty marked at pivotal point of flap. B, Flap in place. C, Healing of flap resulted in distortion of vermilion border. D, E, Z-plasty performed to correct distorted vermilion border. F, Six months after Z-plasty.
Notching of the nostril margin can result from lacerations of the nostril or after reconstruction of the alar or nasal facet with a local cutaneous flap or skin graft. If the notching is not severe, it can frequently be corrected with Z-plasty (Fig. 27-10). The linear axis of the notch is incorporated into the central limb of the Z-plasty. Triangular flaps with angles of 45° to 60° are marked on either end of the central limb to complete the Z-plasty design. Transposing the flaps releases the contracture of the scar causing the notching. On occasion, insertion of a small cartilage graft beneath the flaps of the Z-plasty may be beneficial in reinforcing the scar lengthening achieved with the Z-plasty.
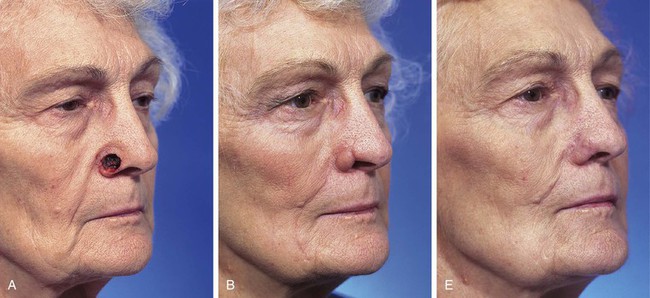


FIGURE 27-10 A, A 1.5 × 1.5-cm skin and soft tissue defect of ala. B, Four months after reconstruction. Ala repaired with auricular cartilage graft for structural support and interpolated melolabial flap for external cover (see Chapter 18). Notching of nostril margin has occurred. C, D, Z-plasty performed to correct deformity. E, Four months after Z-plasty.
A common use of Z-plasty is for release of scar contractures. Scar contractures can result from any cutaneous surgery. Severe contractures may occur in scars resulting from burns or deep skin injury from the use of laser or chemical peels. Z-plasty is frequently employed in the treatment of burn scars of the neck to release contractures that impair movement of the head and neck. Frequently, multiple Z-plasties are required (Fig. 27-11). Chapter 14 is devoted solely to the subject of Z-plasty.



W-Plasty
Like Z-plasty, W-plasty is another method of converting a scar with a regular configuration into one with an irregular pattern. A W-plasty consists of uniform interposed triangular advancement flaps (Fig. 27-12).17,22 It creates a recurring irregularly patterned scar that is less likely to be noticed by an observer’s eye. W-plasty creates a scar that avoids sharp demarcation between scar and adjacent skin by interdigitating small triangles of normal unscarred skin, which has the effect of camouflaging the scar. W-plasty may also be helpful in aligning scars to more nearly approximate the direction of RSTLs of the face.23 It is indicated for scars of the forehead, eyebrow, temple, nose, cheek, and chin that are oriented 35° or more from RSTLs (Fig. 27-13).24 W-plasty is frequently effective in improving the appearance of scars over a convex facial contour. Examples are scars located along the mandibular border, the anterior surface of the ear, and the central forehead.7,17,22
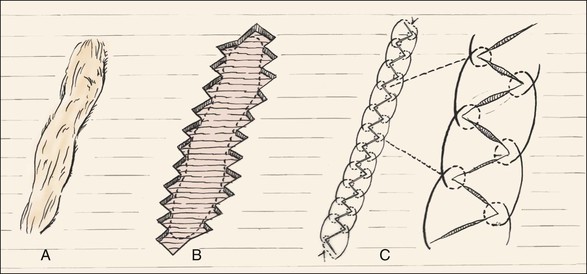
FIGURE 27-12 A, Scar perpendicular to RSTLs. B, W-plasty performed by designing repeating triangular flaps roughly parallel to RSTLs on either side of scar. Scar excised and flaps interdigitated. C, Wound closure with interrupted buried dermal sutures and running locked 6-0 rapidly absorbing gut suture.

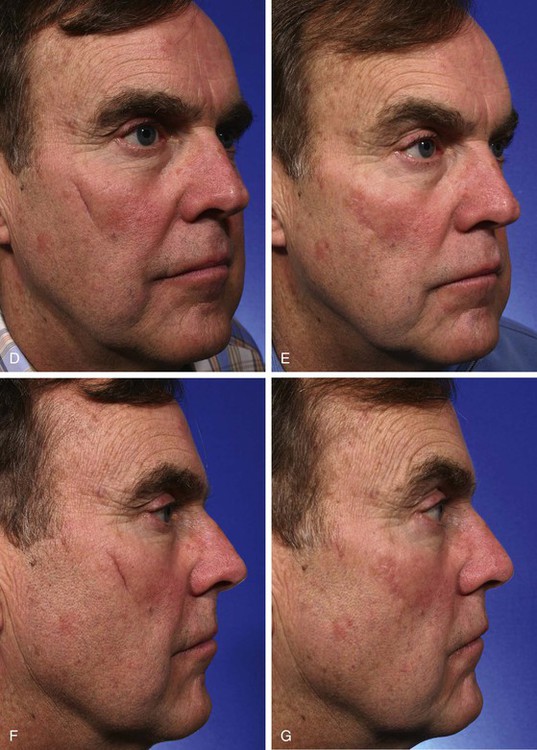
FIGURE 27-13 A, W-plasty designed to revise cheek scar. B, C, Scar excised and W-plasty completed. D-G, Preoperative and 2-month postoperative views.
In performing a W-plasty, the scar should be outlined and RSTLs should be marked where they cross the scar. The orientation of the triangular flaps of the W-plasty is parallel to the RSTLs or slanted in the direction of the RSTLs.17 A series of Ws are drawn so that the apices of the triangles are 5 to 7 mm peripheral to the scar (Fig. 27-14); 3 mm or less tends to be too small to irregularize the scar sufficiently to prevent it from appearing as a straight line, and limbs of more than 7 mm are sufficiently long that the limbs of the flaps create a scar that is individually visible. A mirror image of the first side is drawn on the opposite side of a scar so that the tips of the triangular flaps will interdigitate when the skin is advanced perpendicular to the direction of the scar. Angles of the W-plasty should be designed to be at least 60° to allow adequate tissue interposition, optimal vascularity with minimal tip of flap edema, and interposition of tissue that will resist scar contracture.3,7 A M-plasty can be used at the end of the scar to prevent extension of the incision. Incisions should be made with a No. 11 scalpel blade. Mature subdermal scar tissue is left in situ to help resist contracture and depression of the scar during healing. Wide undermining of the borders of the incisions is performed. The wound is approximated in layers. The cutaneous suture may be a running locking or interrupted suture of nylon or 6-0 fast absorbing gut. Exact alignment of the epithelial surface is critical. The wound is reinforced with paper tape for 1 week. The greatest disadvantage of W-plasty is that it creates a scar that is predictably irregular, so when a long scar is revised, it may result in a new scar that is still readily detected by an observer. Thus, for very long scars (more than 4 cm), a geometric broken-line closure is recommended.

FIGURE 27-14 A, Unsightly scar from rotation flap. Superior portion of scar is perpendicular to RSTLs. B, Superior portion of flap contoured concomitant with W-plasty scar revision. Persistent standing cutaneous deformity excised inferiorly. C, D, Scar excised and W-plasty completed. E, Postoperative result at 1 year.
Geometric Broken Line
The greatest disadvantage of W-plasty scar revision is that the procedure creates a predictably irregular scar. Thus, long W-plasties may cause a scar to be more detectable than if a geometric broken-line scar revision is performed. A geometric broken-line scar revision consists of a series of random, irregular geometric shapes incised along one border of the scar with the mirror image of this pattern incised on the opposite border (Fig. 27-15). The randomness of the design causes the scar to be more difficult for the observer’s eye to follow, thus having the effect of scar camouflage. The geometric broken line is most useful for treatment of scars that are long and linear and cross RSTLs (Fig. 27-16). Similar to W-plasty, each geometrically shaped component of a geometric broken-line scar revision should measure 3 to 7 mm in length.22 Much of the scar created by the geometric broken-line technique will not parallel RSTLs. Rectangle-shaped components should be interspersed with other angular shapes to prevent circular scar contraction. To reduce trap-door deformity, the use of curved components should be limited (Fig. 27-17). Similar to W-plasty, the superficial portion of the scar is excised, leaving the deep dermal and subdermal scar in situ. The surrounding borders of the excised scar are widely undermined, and the geometrically shaped skin edges of the wound are carefully opposed so that the corresponding geometric shapes fit precisely together. A two-layered wound closure is always performed.
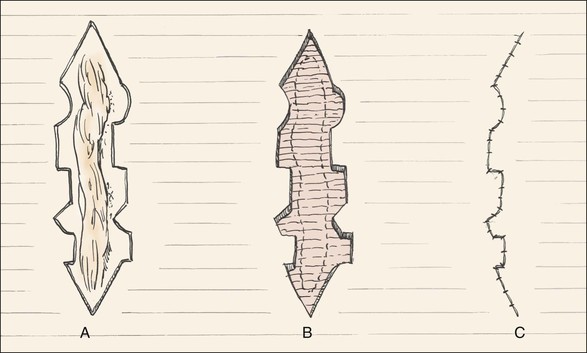
FIGURE 27-15 Geometric broken-line scar revision. A, Random geometric figures designed on either side of scar. B, Scar excised, leaving mirror-image wound edges. C, Wound edges advanced and approximated with running locking 6-0 rapidly absorbing gut suture.
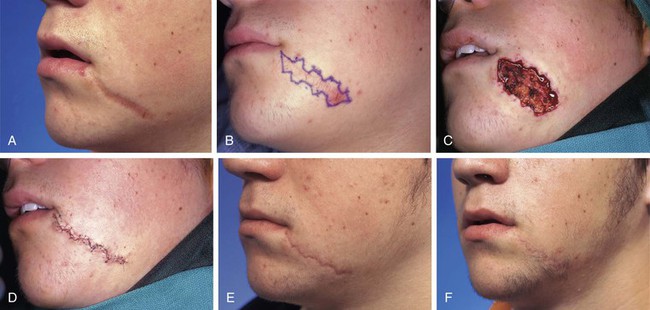
FIGURE 27-16 A, Wide unsightly scar not parallel to RSTLs. B, Geometric scar revision designed. Geometric shapes mirror each other on either side of scar. C, Note how wound spreads when contracted scar is excised. D, Wound approximated. E, Postoperative result at 4 months immediately before dermabrasion. F, Postoperative result at 10 months.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


