Summary and Key Features
- •
Scar formation occurs as a result of cutaneous injuries affecting the dermis and can negatively impact patients’ quality of life.
- •
Significant variability remains in post-operative steps taken by healthcare practitioners to address scarring. No single scar management method is widely used.
- •
Silicone gel sheets and silicone gels have the strongest evidence of support for improving scars, by decreasing fibroblast activity and improving wound hydration, enhancing overall scar texture, color, and appearance.
- •
Other topical treatments including onion extract, topical corticosteroids, topical calcipotriol, and vitamin E have limited evidence to support use in scar cosmesis.
- •
Petrolatum ointment remains a widely recommended and effective agent for wound healing and improving scar cosmesis due to its hydrating effects.
- •
Further research is needed to investigate scar cosmeceuticals in varying skin types and to explore other treatment modalities.
Introduction
Scars are a common problem that affects almost every patient’s skin. Whether occurring by injury, biopsy, or surgery, any cutaneous injury affecting the dermis will heal with a scar. Scars can cause a myriad of symptoms including dryness, pruritus, and tenderness in addition to being cosmetically bothersome, thereby negatively impacting patients’ quality of life. Although every healthcare practitioner hopes to limit scar development in their patients, significant variability among dermatologic practices remains on the steps taken postoperatively to address scarring, with some practices not addressing scar prevention techniques at all.
While no single, widely used scar management method has been established, several topical treatments have demonstrated efficacy for improvement of scar cosmesis, by improving their texture, color, and overall appearance. Silicone gel sheets and silicone gels appear to have the strongest evidence to support improvement, although silicone additives, onion extract, topical corticosteroids, vitamin E, petrolatum ointment, and other emerging therapies have been described. This chapter reviews the available evidence for different scar cosmeceuticals and provides recommendations on topical treatment for improved scar cosmesis. Other modalities used for the treatment of scars including pressure and massage therapy, intralesional injections, lasers, and surgery are excluded from this chapter.
Pathophysiology of Wound Healing
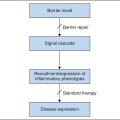
Wound healing is a complex process driven by an orchestra of cellular processes and numerous cytokines. The steps of wound healing are typically divided into three phases: the inflammatory phase, the proliferative phase, and the maturation phase. The inflammatory phase, which lasts approximately 72 hours from injury, begins with the formation of a platelet plug and the coagulation cascade. Neutrophils at this stage phagocytize dead tissue and produce free radicals to kill bacteria in the wound, as well as secrete key proinflammatory cytokines. Monocytes arrive next and differentiate into macrophages, which conduct a number of important functions in wound healing and play a key role in overall wound homeostasis. The proliferative phase occurs next, at days 4–21, and involves angiogenesis, formation of extracellular matrix, and epithelialization. Fibroblasts produce granulation tissue, transform into myofibroblasts to promote wound contraction, and help stimulate keratinocytes for reepithelialization. The final stage, maturation, occurs at around 3 weeks, may last up to 1 year, and is notable for collagen remodeling and wound contraction. The ability to cease ongoing collagen production, with maximum deposition at 21 days, is a hallmark of normal wound healing physiology. Disruptions to the homeostasis of the wound-healing process are believed to contribute to aberrant scar formation. Although the exact pathophysiology of hypertrophic scars and keloid scars is not known, it is believed that prolongation of the inflammatory phase and excessive fibroblast activity and collagen deposition are involved in the formation of both scar types.
Scar Cosmeceuticals
Silicone Gel and Silicone Gel Sheets
Silicone gel sheets are semiocclusive adhesive films of silicone that can be applied onto immature scars for 12–24 hours per day starting 1 week after surgery. Silicone gels are gel formulations that can be applied topically twice daily to immature scars. One study prepared a model of dermal skin with fibroblast cultures grown within collagen lattices, which were then treated with several brands of silicone sheeting versus Saran Wrap for 5 days. Fibroblast activity and fibrogenic cytokine transforming growth factor beta-2 (TGF-β2) were both decreased in the silicone-treated group, and the silicone-treated group had objectively less contraction compared to the Saran Wrap control group. This suggests silicone gel may improve scar formation by decreasing fibroblast activity, a key component believed to contribute to hypertrophic scars. Other studies have demonstrated silicone may increase the temperature of immature scars and improve hydration of the wound, which assists the migration of keratinocytes into healing wounds.
Clinical studies evaluating the efficacy of silicone gel sheets have shown improved scar cosmesis. A systematic review of 10 trials evaluating silicone gel sheeting and silicone gel compared to the control group found a statistically significant difference between silicone gel sheeting and placebo in preventing hypertrophic scar formation. The review article did note, however, that many of the studies were of poor quality with high or uncertain risk of bias. A systematic review of 20 trials evaluating silicone gel sheeting for prevention or treatment of hypertrophic or keloid scars compared with no treatment found weak evidence of benefit of silicone gel sheeting as a prevention for abnormal scarring in high-risk individuals. The review added again that poor quality of research means a lot of uncertainty remains. There may also be added benefit of silicone gel sheets for those at high risk of developing hypertrophic or keloid scars, as one study found.
Silicone gel appears to be a useful modality for scar prevention as well. In a randomized controlled trial of 110 patients undergoing surgery at an outpatient dermatologic office, silicone gel was compared with zinc oxide cream over a 6-month treatment period. Scar alterations (defined as keloidal, hypertrophic, diastasic, or atrophic) were significantly more common in the control group (55% of patients) compared to the silicone gel group (27% of patients). Additionally, 11% of patients in the control group developed keloids, whereas no patients in the treatment group developed keloids. A metaanalysis found that, when compared head-to-head, there was no difference in efficacy between silicone gels and silicone gel sheets.
Silicone gel sheets and silicone gels have the strongest evidence of support for improving scars, with most studies supporting their potential benefit for scar cosmesis. For any patient hoping for the best cosmetic outcomes after dermatologic procedures, the authors recommend use of topical silicone gel or silicone gel sheets for up to 6 months following the procedure to optimize healing and minimize hypertrophic scarring.
Onion Extract
Onion extract is an ingredient in several cosmetic scar creams and gels, such as Mederma (Merz Pharmaceuticals, Frankfurt, Germany). The active ingredient, allium cepa , has been shown to upregulate matrix metalloproteinase-1 (MMP-1) activity and inhibit fibroblast activity, both acting as mediators to reduce excess collagen and scar formation. In a randomized controlled trial comparing onion extract to no treatment for new dermal scars in 44 patients following dermatologic surgery, those treated daily with onion extract gel for 8 weeks were rated significantly improved from baseline by both the subjects and the investigators, compared to the control scars. This study did, however, also note an increased rate (13.6%) of burning, stinging, and contact dermatitis in the gel-applied scars compared to the control scars. Although there was noted improvement in this study with use of onion extract, this study was at high risk for observer bias, and the incidence of contact dermatitis would be an important consideration when choosing this agent for scar treatment.
In contrast, another study comparing onion extract versus petrolatum-based ointment in 17 patients 1 month after Mohs surgery found no significant improvement in scar appearance or symptoms between the two groups. This suggests that petrolatum-based ointment, which is considered to improve scar cosmesis primarily by hydration, was equally effective compared to onion extract and raises the question of onion extract’s efficacy in improving scar cosmesis.
Although there are conflicting data on the efficacy of onion extract used in isolation for improvement of scar cosmesis, onion extract combined with silicone gel does appear to have synergistic benefit for scar prevention. In a double-blind pediatrics study of 10% onion extract in silicone gel versus silicone gel alone, the onion extract–silicone gel combination showed statistically significant improvement in preventing significant scars and preventing hypertrophic scars. Other, similar studies comparing silicone gel or standard wound care versus silicone gel–containing herbal extracts (including onion extract) suggested scars at 6-month follow-up had better cosmetic outcomes when using silicone gel containing onion extract. This suggests that combination modalities including silicone and onion extract may have improved outcomes for scar cosmesis.
Considering the varying results from studies evaluating onion extract on improving scar cosmesis, whether alone or in conjunction with other modalities such as silicone, there is weaker overall evidence to support onion extract use alone for the treatment of immature scars.
Vitamin E
Vitamin E has been investigated as an adjunct to silicone gels and as a stand-alone concentrate for improvement of scar cosmesis. Vitamin E is lipophilic and suspected to absorb through cell membranes and serve as an antioxidant to eliminate free radicals. Vitamin E has been proposed to aid in wound healing by reducing fibroblast proliferation and inflammation.
One randomized clinical trial comparing vitamin E and petrolatum-based emollient suggested there may be some benefit for use of vitamin E in treatment of skin 15 days before and 30 days after surgery in the pediatric population. However, other studies have shown limited benefit of vitamin E on improving scar cosmesis. A study of patients following Mohs surgery treated with Aquaphor versus Aquaphor combined with vitamin E found there was no significant improvement in cosmetic appearance of surgical scars. Furthermore, 33% of patients in this study treated with vitamin E developed contact dermatitis, which was not observed in the control group. Other studies have similarly shown little benefit with vitamin E alone for scar prevention, but some have shown improvement of scar outcomes when used as an additive to silicone gel.
Overall, the authors feel the current evidence does not support the use of vitamin E in scar prevention therapy, and the risk of contact dermatitis with this agent further dissuades the authors from its use in postoperative care for scar cosmesis.
Topical Corticosteroids
Although intralesional injections of steroids are beneficial for reducing scarring, topical corticosteroids have not shown to be beneficial in clinical trials for scar prevention and wound healing. When applied topically, steroids do not penetrate deep enough in a high enough concentration to be beneficial in inhibiting fibroblast activity, suppressing inflammation, or reducing excess collagen deposition. Topical steroids likely do not harm wound healing but are not recommended for improvement in scarring cosmetic outcomes.
Calcipotriol
Topical vitamin D treatments have been efficacious for treating inflammatory conditions, such as psoriasis. However, the topical treatment has not been shown to be effective in preventing hypertrophic scarring in randomized controlled trials. Thus this agent is not recommended for use in topical therapy to improve scarring.
Petrolatum Ointment
Despite the growing number of newer wound healing agents and scar cosmeceuticals, perhaps the most established agent, and thus one that deserves mention in this review, is petrolatum-based ointment, with common examples including Vaseline and Aquaphor. Petrolatum ointment remains the most recommended agent to aid with wound healing following dermatologic surgery. A study evaluating 169 individual dermatology wound care handouts found that 84% recommended application of petrolatum-based products following surgery, specifically Vaseline (75%) and Aquaphor (43%). Indeed, petrolatum-based products have become the standard in many dermatology practices and continue to be considered an effective agent for wound healing. The presumed mechanism for petrolatum is improved hydration, which can assist with the migration of keratinocytes into healing wounds. To our knowledge there are no studies specifically comparing petrolatum ointment to no topical treatment; however, it has been used for decades now as a standard of care following many dermatologic procedures. Furthermore, many of the studies evaluating newer scar cosmeceuticals use petrolatum ointments as the control agent, and in some cases petrolatum ointments perform just as well as the newer agents being tested.
Overall, the authors feel this agent continues to remain an effective tool for early stages of wound healing and improving scar cosmesis, with the added benefits of low cost and wide tolerability by patients.
Targeting Inflammatory Mediators and Interleukins
The latest science on scar reduction has begun investigating the role of inflammatory factors such as growth factors and interleukins on wound healing and scar formation, in some cases having implications on treatment. For instance, studies have found an overproduction of TGF-β and suppression of prostaglandin E2 (PGE2) in excessive wound scarring compared with normal wound healing. In one study, keloid fibroblasts were found to produce less PGE2 than control fibroblasts, suggesting that the observed increased collagen synthesis in keloid fibroblasts might be attributed to decreased PGE2. Nonsteroidal antiinflammatory drugs (NSAIDs) and their selective cyclooxygenase-2 (COX-2) inhibitors, which are frequently taken by patients for pain relief and treatment of other inflammatory conditions, inhibit PGE2 production. Therefore NSAIDs have been proposed to exacerbate excessive scar formation.
Interleukins, which play a prominent role in initiation of inflammation and likely of subsequent proliferation and remodeling, are being investigated as factors involved in wound healing and scar formation. Interleukin-6 (IL-6) and IL-1β, proinflammatory factors, have been proposed to play an important role in promoting scar formation, while IL-10 has been proposed to act as an antiinflammatory factor in wound healing. IL-4 and IL-13 were found to be increased in some pathological scars, and in one study dupilumab, a monoclonal antibody against IL-4Rα, had an inhibitory effect on keloids. Other interleukins involved in wound healing and scar formation are being investigated in ongoing studies, and future treatment modalities targeting these specific factors may be on the horizon.
Other Treatments
Several other topicals have limited evidence investigating their benefit for scar prevention. Topical losartan, topical timolol, topical liposome-encapsulated statins, topical naltrexone, and topical 1,4-diaminobutane are medications with benefit in single-case studies. Given the paucity of data available, none of these topical treatments are recommended at this time to be incorporated into wound healing regimens.
Conclusion
Wound healing occurs by a complex array of cellular pathways, with variable outcomes in final scar formation among patients, in many cases having an impact on their quality of life. Knowledge of these wound-healing pathways aids in the understanding of scar pathophysiology in addition to understanding the mechanism of action of various proposed scar cosmeceuticals. Early intervention with scar cosmeceuticals may help in improving final scar cosmesis. Overall, silicone gel sheets and silicone gel appear to have the most supportive evidence for improving wound healing and final scar outcomes. Other agents such as onion extract, vitamin E, topical corticosteroids, and calcipotriol have less evidence supporting their utility. The available literature examining scar cosmeceuticals has not been stratified by Fitzpatrick skin types; meanwhile differences in skin collagen formation among different skin types have been shown. Further research is needed to investigate existing scar cosmeceuticals in varying skin types. Other treatment modalities for wound healing and scars, such as intralesional injections, lasers, and surgery, were not addressed in this chapter but may be of utility in combination with the topical agents that have been reviewed here.
Further Reading
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


