Summary
Very vascular, proceed with caution during in-office procedures.
There is very little laxity, especially on the vertex.
Scalp will tolerate significant tension on closure.
For exposed calvarium, simple bone burring and split-thickness skin grafting will not result in durable coverage.
Temporary alopecia with repairs is common but rarely permanent.
10.1 Algorithm For Closure (▶ Fig. 10.1)
10.1.1 General Considerations
Although appropriate scalp reconstruction techniques will be rewarded with a healed aesthetically pleasing scalp, care and caution should be exercised in planning and execution. The scalp is exceedingly vascular, which lends itself to reliable reconstruction with low risk of infection. However, this vascularity can increase risk of significant bleeding during the Mohs resection, intraoperative repair, and postoperatively, and requires that diligent care and precautions be made. 1, 2, 3 A patient may have suffered a significant amount of bleeding in the Mohs surgeon’s office prior to presentation for surgical repair and the possibility of a low hemoglobin in an elderly patient with cardiac compromise should always be considered. Diligent preoperative hemodynamic monitoring and hemoglobin measurement, if indicated, should be practiced. Also, understand during preoperative planning that there is very little scalp laxity in closure and decision making regarding techniques should both be planned with a good deal of precision, and that the next step, or lifeboat, needs to be considered and available. For this reason, it is prudent to treat even what would be considered the most trivial scalp defects in an operative setting. They do not often require general anesthesia; however, the safety and monitoring that is available in the operating room versus an office is preferable. The scalp itself can tolerate significant tension on closure and our general rule of thumb in a patient with no other morbidities is that if the closure can be maintained with skin staples, it will ultimately continue on to healing.
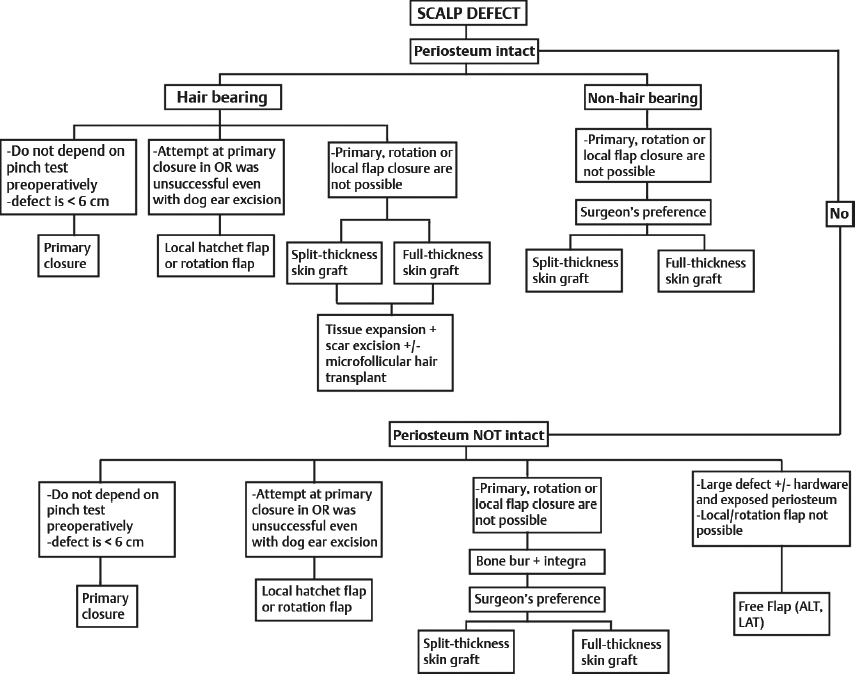
Fig. 10.1 Algorithm for scalp reconstruction.
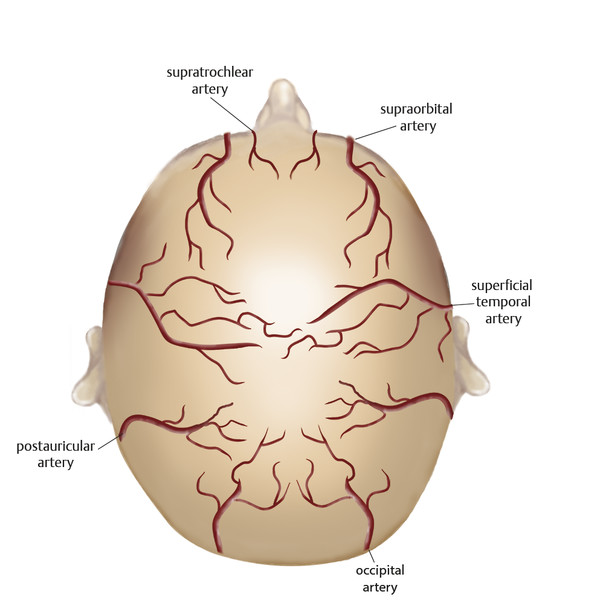
Fig. 10.2 Blood supply of the scalp.
The general concept of scalp reconstruction and decision making can be greatly simplified by the consideration of both the defect starting point and the ultimate final endpoint for the patient. This consists simply of the defect starting point being with either periosteum intact or not and the defect endpoint being hair-bearing scalp or simple soft-tissue coverage. An example of this is if the periosteum is intact and the endpoint is not hair-bearing coverage, any scalp defect can be simply covered with a split-thickness skin graft (STSG) for final definitive coverage. If either the endpoint or the starting point is different from this, then multiple other factors go into the management decision. For hair-bearing scalp coverage, the options range from direct closure, local flap closure, or initial STSG with tissue expansion placement and alopecia excision on the way to final hair-bearing coverage or soft-tissue coverage followed by microfollicular hair transplantation (▶ Fig. 10.2).
10.2 Commonly Applied Methods of Closure
Assistive wound healing agents (Integra or ACell) with or without bone burring and skin grafting.
Primary closure.
For larger defects, rotation flaps may be employed, particularly for hair-bearing scalp.
Full- or split-thickness skin graft coverage either directly or proceeded by Integra placement.
For large defects without intact periosteum or with exposed hardware, free tissue transfer remains the gold standard.
10.2.1 Bone Exposure and Calvarial Defects
The common perception that exposed bone and calvarial defects can be managed with simple bone burring and split-thickness graft coverage is not entirely correct. This technique rarely results in a permanently closed wound and often results in chronic wound breakdown, continued intermittent bone exposure, and risk for serious complications such as skull osteomyelitis. 4 With the advent of bilaminar dermal matrices, management of these previously difficult defects has been made much safer and more predictable. 5, 6, 7
10.2.2 Direct Closure
We manage most scalp wounds with direct closure. The preoperative “pinch test” is notoriously inaccurate for determining the ability to be closed directly. Usually, we limit this to 4-cm defects, again restricted by the patient’s laxity, but remember, simply pinching the inelastic scalp together while the patient is awake is not an accurate assessment. 3, 8 The thick remaining scalp tissue that comprises the dog-ear extent of the wound will restrict the final closure until excised in the operating room (▶ Fig. 10.3).

Fig. 10.3 A 36-year-old white male status post 4 × 3.5 cm Mohs excision for basal cell carcinoma on scalp vertex. Wound was repaired with primary closure with standing cone excision. Postoperative results shown at 7 months.
When it is uncertain whether or not the defect will be able to be closed directly, an algorithm to follow is to leave the option of local flap closure, in this case a hatchet flap closure—by simply incising one of the contralateral opposing limbs of the hatchet flap and attempting to close the scalp directly. If the scalp does not close and is left with a central defect, then simply rotate the V-Y hatchet flaps into position and this will serve as soft-tissue coverage, although the scar pattern will not be as ideal as it would if the wound is able to be closed directly. Other adjuncts available to facilitate a direct wound closure include wide undermining and galeal scoring. Galeal scoring is performed with a no. 15 blade or pinpoint cautery taking care to just incise the galea without damaging the more superficial vessels. 9, 10 This will provide a mathematical tissue advancement (see ▶ Fig. 10.4). 9, 11 With these three techniques, the majority of small (up to 4 cm) scalp defects can be closed directly. Remember, if the wound edges can be maintained in opposition with a standard skin stapler, the incision will likely proceed on to healing (▶ Fig. 10.4, ▶ Fig. 10.5, ▶ Fig. 10.6).
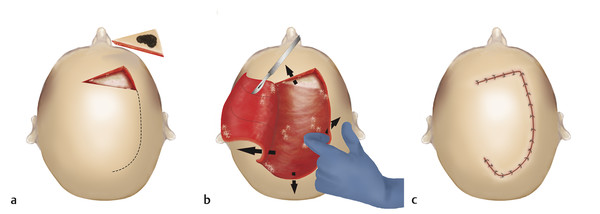
Fig. 10.4 (a) Removal of lesion in wedge shape to facilitate rotational closure; (b) galeal scoring and undermining of rotation flap (undermining indicated by arrows) to maximize advancement; (c) final postoperative closure.
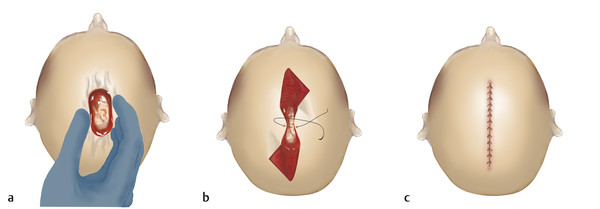
Fig. 10.5 (a) Preoperative pinch test, often inaccurate to determine whether or not a wound can be closed directly on the scalp; (b) partial excision of standing cones to evaluate whether or not wound may be closed linearly; (c) final appearance with linear closure.
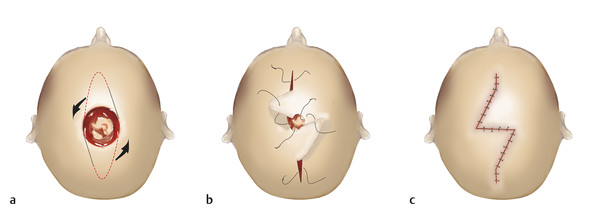
Fig. 10.6 (a) When intraoperative attempts at primary closure prove unsuccessful, standing cones can be converted to a “hatchet flap” design after partial incision and demonstration that linear closer is not an option; (b) the standing cones are then rotated inward to cover defect; (c) final postoperative appearance.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


