Rosacea
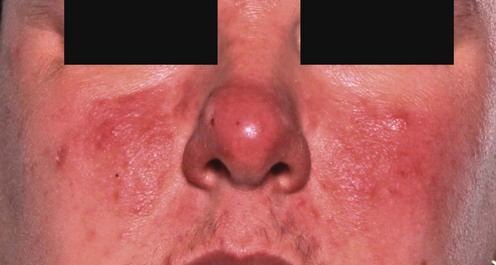
Inflammatory rosacea
First-line treatments
 Topical metronidazole
Topical metronidazole
A
 Topical azelaic acid
Topical azelaic acid
A
 Oral tetracyclines
Oral tetracyclines
A
 Oral erythromycin
Oral erythromycin
C
 Emollients
Emollients
C
Second-line treatments
Third-line treatments
 Systemic isotretinoin
Systemic isotretinoin
B
 Topical tretinoin
Topical tretinoin
C
 Topical adapalene
Topical adapalene
B
 Topical sulfur
Topical sulfur
B
 Topical corticosteroids
Topical corticosteroids
D
 Topical ketoconazole
Topical ketoconazole
D
 Systemic ketoconazole
Systemic ketoconazole
D
 Topical bifonazole
Topical bifonazole
D
 Photodynamic therapy
Photodynamic therapy
D
 Spironolactone
Spironolactone
D
 Demodex eradication
Demodex eradication
B
 Helicobacter pylori eradication
Helicobacter pylori eradication
D
 Sunscreens
Sunscreens
E
 Topical tacrolimus
Topical tacrolimus
C
 Topical pimecrolimus
Topical pimecrolimus
D
 Octreotide
Octreotide
C
 Inhibition of ovulation
Inhibition of ovulation
C
 Topical NADH
Topical NADH
C
 Topical 1-methylnicotinamide
Topical 1-methylnicotinamide
C
 Oral nicotinamide with zinc
Oral nicotinamide with zinc
C
 Zinc sulphate
Zinc sulphate
B
 Trichloroacetic acid peels
Trichloroacetic acid peels
E ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Rosacea


 Topical erythromycin
Topical erythromycin Topical clindamycin
Topical clindamycin Oral metronidazole
Oral metronidazole Topical benzoyl peroxide
Topical benzoyl peroxide Ampicillin
Ampicillin Azithromycin
Azithromycin