Melanoma is an important public health problem in the United States and worldwide. The incidence of melanoma continues to increase at a high rate and deaths from melanoma are also increasing. The endogenous risk factors that are currently recognized are in many cases surrogates for genetic markers yet to be determined. Exogenous risk factors need to be better defined and understood to help develop better public education programs that can change risk behaviors and subsequently lower future incidence and mortality from melanoma.
- •
Melanoma is an important public health problem in the United States and worldwide.
- •
Factors that increase the risk of developing melanoma are:
- ○
History of blistering sunburns as a teenager
- ○
Red or blonde hair
- ○
Marked freckling of upper back – sign of excessive sun exposure and that a person is susceptible to it
- ○
Family history of melanoma
- ○
History of actinic keratoses (AKs) – considered the earliest stage in the development of skin cancer
- ○
Intermittent high intensity sun exposure.
- ○
- •
Exogenous risk factors need to be better defined and understood to help develop better public education programs.
Introduction
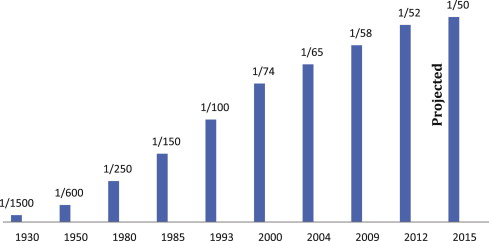
Melanoma is an important public health problem in the United States and worldwide. The incidence of melanoma has been increasing faster than that of any other cancer in the United States. Overall, melanoma incidence increased 2.9% annually from 1981 to 2006. Statistically significant increases are occurring for tumors of all histologic subtypes and thicknesses, including those greater than 4 mm. Invasive melanoma currently is the fifth most frequently diagnosed cancer in men and the sixth most frequently diagnosed cancer in women in the United States. In 2012, 76,250 newly diagnosed cases of invasive melanoma and 55,560 cases of in situ melanoma were expected. At current rates, the lifetime risk of an American developing invasive melanoma is 1 in 52 ( Fig. 1 ) overall, 1 in 38 for Caucasian men, and 1 in 56 in Caucasian women. This rate contrasts dramatically with a lifetime risk of 1 in 1500 for Americans born in 1935. Approximately 9180 people are expected to die from melanoma in the United States during 2012, accounting for 66% of all deaths caused by skin cancer.
The importance of diagnosing melanoma early in its evolution cannot be understated. Because the primary treatment modality of cutaneous melanoma, surgical excision, has not changed substantially over the past several decades, the improved 5-year survival rate can be primarily attributed to earlier detection. There has been steady improvement in survival from melanoma over decades with the 5-year survival for invasive melanoma increasing from 82% in 1979 to 92% in 2002. Early detection depends on recognition and identification of patients at high risk for the development of melanoma.
The factors that significantly influence a person’s risk of developing melanoma are discussed subsequently.
Natural UV light exposure (sunlight)
Exposure to UV radiation from the sun is the most important environmental risk factor for the development of melanoma. Melanoma risk strongly correlates with UV exposure and sunburns; the face and neck are common anatomic sites for skin cancer. Exposure to UV radiation on the skin results in clearly demonstrable mutagenic effects. The p53 suppressor gene, which is often mutated in melanoma, is directly affected by UV exposure. The primary wavelengths influencing melanoma risk are most likely in the UV-B (290–320 nm) range. However, animal studies have also demonstrated a small effect on melanoma development due to exposure to UV-A wavelengths. Individuals with type I and II skin types who are more sensitive to the effects of exposure at these wavelengths are at higher risk for the development of skin cancer.
The amount of average annual UV radiation correlates with the incidence of melanoma. The closer an individual is to the equator, the greater the intensity of UV exposure that occurs. The US Surveillance, Epidemiology and End Results (SEER) incidence of melanoma shows a direct relationship between the incidence of melanoma and latitude. The correlation of melanoma incidence to UV radiation exposure is greater when ambient UV-A (320–400 nm) radiation is also included. High-altitude regions have a higher melanoma rate that may be related to the higher UV fluences (J/cm 2 ) noted at these sites. Melanoma risk is directly related to the annual UV exposure. When lifetime residential history was coupled with levels of midrange UV radiation (UV-B flux) to provide a measure of individual exposure to sunlight, a 10% increase in annual UV-B flux was associated with a 19% increased risk for melanoma.
Solar radiation UV photons have direct damaging effects on molecules and cells, including DNA, proteins, and lipids, which cause immunosuppression, photoaging, and photocarcinogenesis. Intermittent recreational exposure to UV has been directly correlated to the increased risk for the development of melanoma.
Natural UV light exposure (sunlight)
Exposure to UV radiation from the sun is the most important environmental risk factor for the development of melanoma. Melanoma risk strongly correlates with UV exposure and sunburns; the face and neck are common anatomic sites for skin cancer. Exposure to UV radiation on the skin results in clearly demonstrable mutagenic effects. The p53 suppressor gene, which is often mutated in melanoma, is directly affected by UV exposure. The primary wavelengths influencing melanoma risk are most likely in the UV-B (290–320 nm) range. However, animal studies have also demonstrated a small effect on melanoma development due to exposure to UV-A wavelengths. Individuals with type I and II skin types who are more sensitive to the effects of exposure at these wavelengths are at higher risk for the development of skin cancer.
The amount of average annual UV radiation correlates with the incidence of melanoma. The closer an individual is to the equator, the greater the intensity of UV exposure that occurs. The US Surveillance, Epidemiology and End Results (SEER) incidence of melanoma shows a direct relationship between the incidence of melanoma and latitude. The correlation of melanoma incidence to UV radiation exposure is greater when ambient UV-A (320–400 nm) radiation is also included. High-altitude regions have a higher melanoma rate that may be related to the higher UV fluences (J/cm 2 ) noted at these sites. Melanoma risk is directly related to the annual UV exposure. When lifetime residential history was coupled with levels of midrange UV radiation (UV-B flux) to provide a measure of individual exposure to sunlight, a 10% increase in annual UV-B flux was associated with a 19% increased risk for melanoma.
Solar radiation UV photons have direct damaging effects on molecules and cells, including DNA, proteins, and lipids, which cause immunosuppression, photoaging, and photocarcinogenesis. Intermittent recreational exposure to UV has been directly correlated to the increased risk for the development of melanoma.
Artificial UV tanning
Approximately 30 million people tan indoors in the United States annually, including 2.3 million adolescents. Despite increased evidence on the dangers of artificial UV radiation, the popularity of indoor tanning is growing. The relationship between UV exposure from tanning beds and subsequent development of melanoma has now been well documented.
More than 20 case-control studies have investigated a possible link between indoor tanning and melanoma. The more recent and more rigorously designed studies have found a positive correlation with an increased risk of melanoma. A study of 571 first time patients with melanoma compared with 913 healthy controls found a significantly higher odds ratio (OR) of 1.8 between indoor tanning and melanoma. In another study of 1518 patients with dermatologic diseases surveyed for skin cancer history and tanning bed use, a significant increased risk of malignant melanoma was noted for every use of indoor tanning (OR 1.64), and a very strong correlation was noted for women aged 45 years or younger who used indoor tanning equipment (OR 3.2). Persons with a history of tanning bed usage and that of melanoma are at increased risk for additional subsequent primaries.
A meta-analysis of 19 studies of indoor tanning and melanoma risk suggested that every use of indoor tanning was associated with the development of melanoma with a relative risk of 1.15, whereas the first use before the age of 35 showed a significantly increased risk of melanoma, with a summary relative risk of 1.75. Based on this study and other studies, the International Agency for Research on Cancer classified UV exposure from tanning beds at its highest carcinogenic risk category (carcinogenic to humans). The National Institutes of Health has also concluded that “Exposure to sunbeds and sunlamps is known to be a human carcinogen based on sufficient evidence of carcinogenicity from studies in human, which indicate a causal relationship between exposure to sunbeds and sunlamps and cancer.” Indoor tanning has also been calculated to be directly associated with deaths due to melanoma.
Nevi
Acquired melanocytic nevi are important markers for the risk of melanoma development. The total number of melanocytic nevi on the whole body is the most important independent risk factor for melanoma, and the risk for melanoma development increases almost linearly with increased numbers of melanocytic nevi. Presence of dysplastic nevi is an additional independent risk factor for the development of melanoma. Studies have demonstrated that dysplastic nevi are reported in up to 34% to 56% of patients with melanoma, and their presence may confer up to a 10-fold increase in the risk of melanoma.
The development of potential precursors to melanoma, such as dysplastic nevi, is inhibited by the regular use of sunscreen. Lower nevus counts were found in children who regularly used sunscreens than those who did not, suggesting that sun protection at an early age might lower the subsequent risk of melanoma.
Personal and family history of melanoma
Approximately 10% of melanomas present in familial clusters. To date, the exact genes that increase melanoma risk have not been fully described. Yet, there is a clear relationship between a prior personal or family history and melanoma risk.
Patients with histories of a previous primary melanoma are at higher risk for developing a second primary melanoma (2.8–25.6). A recent case series calculated the 5- and 10-year risks for developing a second primary melanoma among patients to be 2.8% and 3.6%, respectively.
In 1820, Norris reported the first case of what is now recognized as familial melanoma syndrome, but it was not until 1978, when Clark and Lynch first described families with the familial, atypical multiple mole melanoma (FAMMM) syndrome, which is characterized by the presence of melanoma in first-degree relatives, large numbers of melanocytic nevi (>50–100), and melanocytic nevi demonstrating architectural disorder and atypia. Genetic analysis of FAMMM pedigrees resulted in the identification of 2 high-penetrance susceptibility genes, the cyclin-dependent kinase inhibitor 2A (CDKN2A) on chromosome 19p21 and cyclin-dependent kinase 4 (CDK4) on chromosome 12q14. Mutations in CDKN2A account for approximately 20% to 40% of hereditary melanoma, and 0.2% to 1% of all melanomas. Mutations in CDK4 are rare and have been reported in less than 15 families worldwide, leaving CDKN2A as the most significant melanoma predisposition gene identified thus far.
In a more recent meta-analysis study MC1R gene, which encodes the melanocyte-stimulating hormone receptor, has been identified as a low penetrance melanoma susceptibility gene. Polymorphic variants at this locus behave as the key determinant of red hair and freckling and are established as low-risk melanoma susceptibility genes. Coinheritance of variants in MC1R also increases the penetrance of CDKN2A in families with familial melanoma.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


