Rib-Pectoralis Major Osteomusculocutaneous Flap
M. S. G. BELL
EDITORIAL COMMENT
Both this and the preceding chapter indicate the interest and study given to the vascularization of the ribs. It is clear that when muscle is attached to bone, it also provides blood supply. The bone will bleed from its edges if there is enough vascularized muscle attached to it; however, anatomic studies do indicate that there is more muscle attached if one takes the fifth rib with the pectoralis major muscle in contrast to the sixth one. When taking the fifth rib, however, the arc of rotation will not extend beyond the central portion of the mandible.
The rib-pectoralis major osteomusculocutaneous flap has been used to provide replacement for mandibular defects and lining tissue in the oral cavity, especially for reconstruction of the soft palate, floor of the mouth, and lateral pharyngeal wall (1). It may be used as a pedicle flap or as a free flap.
ANATOMY
Both the fifth and sixth ribs have been used, and each seems to obtain sufficient blood supply from the overlying pectoralis major muscle to allow flap transfer and survival to provide a reasonably reliable composite flap for complicated reconstructions (2, 3). (For details of the muscle anatomy, see Chapter 135.)
FLAP DESIGN AND DIMENSIONS
I have taken a portion of skin up to 15 cm2 for reconstruction of the soft palate, floor of the mouth, and lateral pharyngeal wall. The inferior margin of the cutaneous portion of the pectoralis major flap may be extended below the costal margin by at least 5 cm.
The skin flap should be cut larger than necessary because the bulk of muscle and fat beneath the skin must be accommodated in closure of the mouth defect, and underestimating this area is easy. Because the rib does provide some degree of rigidity, swelling in the area may increase skin tension on the suture line, and a rather redundant flap will minimize this degree of tension. (I believe that development of fistulas in my series of patients may have been, in part, a result of this problem.)
The cutaneous portion of the flap always should be planned so that the superior margin begins as high as possible to include the perforating musculocutaneous arteries along the lower margin of the pectoralis major muscle. In female patients in whom the inframammary fold must be taken as the upper margin of the skin flap, dissection may be beveled upward, just beneath the breast tissue, preserving cutaneous perforating vessels that may be seen running obliquely downward. This factor may be critical in preserving the cutaneous blood supply.
Either the fifth or sixth rib can be used. In 21 of my 22 patients, the sixth rib was taken. In the reconstruction in which the fifth rib was used, the muscle pedicle was under a little greater tension than with sixth-rib flaps. The fifth-rib flap is useful when an external skin and lip defect also must be covered because a longer skin component can be used.
Access to the base of the pectoralis major flap may be achieved in several ways. A vertical incision is used by many surgeons, with the incision running downward from the mid-portion of the clavicle to the point at which the cutaneous portion of the pectoralis major flap is raised. Access to the flap also may be gained by raising a standard deltopectoral flap. This procedure displays the entire clavicular origin of the muscle and the musculotendinous junction in the axilla, which is subsequently divided.
Access to the sternal origin of the pectoralis major flap is gained by raising a laterally based flap about 10 cm wide at the level of the anterior axillary line that extends medially to the sternum. This flap usually contains the nipple and is designated so that its inferior limb runs right along the proposed skin flap to be carried into the mouth (Fig. 196.1A and B). The amount of skin undermining with this technique is greater than in the vertical incision technique; however, the standard Bakamjian flap is preserved and may be used for help in closure of the chest defect when a large flap is taken. It also may be used for closure of the neck skin should a defect be present there or should a subsequent complication require use of a local flap.
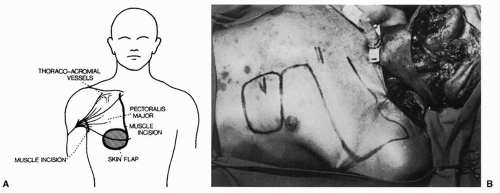 FIGURE 196.1 A: The pectoralis major osteomusculocutaneous flap using a vertical incision for access (see text for details). B: Variation in design to preserve a deltopectoral flap for either immediate or later use. (From Bell, Barron, ref. 1, with permission.) |
OPERATIVE TECHNIQUE
The pectoralis major muscle is raised from the chest wall along its lateral margin. There is a discrete fascial plane allowing blunt dissection. The sternal and clavicular origins of the pectoralis major muscle are separated, and the vessels entering the deep surface of the muscle are easily seen and preserved. The sternal portion of the muscle that will carry the skin and bone is defined laterally to its musculotendinous junction in the axilla.
The muscle is divided at this point (Fig. 196.1). The sternal origin of the muscle then is divided with the cutting cautery. At this point, the rib with the largest muscular attachment can be chosen The skin flap overlying the rib is incised, and the intercostal muscles above and below the rib that are to be taken are divided with the cutting cautery. Periosteum of the rib is preserved to ensure maximum blood supply. The costal cartilage is disarticulated at the sternum, and the rib is divided laterally according to the bone length required. The angle of the costochondral junction, especially in the sixth rib, corresponds well to the angle between the body and vertical ramus of the mandible. The intercostal artery is ligated where it leaves the internal mammary artery, anterior to the thoracis internus muscle.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


