Mestizo patients are the largest ethnic minority in the United States; the main facial plastic procedure they request is rhinoplasty. Mestizo noses are a challenge. It is common to find bulbous, undefined nasal tips sitting on a poorly structured osteocartilaginous framework. A structural approach is presented whereby support structures of the nose are strengthened and reinforced with structural grafts. A gradual approach to the nasal tip is presented whereby sutures and grafts are used to improve rotation and projection and create more definition. Cases showing long-term results are presented with discussion of the different surgical techniques used.
Key points
- •
Rhinoplasty in Mestizo patients is evolving from reductive aggressive techniques to those whereby a structural stepwise approach is used.
- •
Mestizo patients want smaller noses that look more defined, while retaining ethnic features.
- •
The structural technique involves using sutures and grafts to give additional support and create definition with minimal tissue resection.
- •
Structural grafting involves using cartilage grafts as devices that give additional support to underlying support structures of the nose.
- •
Sutures are an excellent alternative to increase rotation and create definition without decreasing the support of the nasal tip.
Introduction
More than half of the growth of the population of the United States from 2000 to 2010 was due to an increase in the Hispanic population. Even though today Hispanics are not the fastest growing ethnic group within the United States, they still are the biggest ethnic minority, making it a very important group of patients seeking facial plastic surgery procedures.
Rhinoplasty is the leading facial plastic procedure that is performed worldwide and Latin America is not an exception. Today there is an increasing awareness that rhinoplasty is not a “one-size-fits-all” procedure and more often more patients are looking for specialists who have experience in dealing with ethnic patients and their particular problems.
The trends in rhinoplasty surgery have also shifted from the traditional reductive aggressive procedures to those wherein ethnic features are preserved. Mestizo patients are not the exception. A structural stepwise approach is presented whereby satisfactory long-term results can be achieved using sutures and graft to reinforce support structures and define nasal features.
Introduction
More than half of the growth of the population of the United States from 2000 to 2010 was due to an increase in the Hispanic population. Even though today Hispanics are not the fastest growing ethnic group within the United States, they still are the biggest ethnic minority, making it a very important group of patients seeking facial plastic surgery procedures.
Rhinoplasty is the leading facial plastic procedure that is performed worldwide and Latin America is not an exception. Today there is an increasing awareness that rhinoplasty is not a “one-size-fits-all” procedure and more often more patients are looking for specialists who have experience in dealing with ethnic patients and their particular problems.
The trends in rhinoplasty surgery have also shifted from the traditional reductive aggressive procedures to those wherein ethnic features are preserved. Mestizo patients are not the exception. A structural stepwise approach is presented whereby satisfactory long-term results can be achieved using sutures and graft to reinforce support structures and define nasal features.
The Mestizo patient
Mestizo means mixture of races. It is a combination of the local Indian tribes that inhabited the different regions of the continent, the Europeans (mainly Spanish invasions) who initially conquered the area in the fifteenth century, and the Africans that were brought over during the slave trade ( Fig. 1 ). Additional European migrations during the first and second World Wars complete the picture.
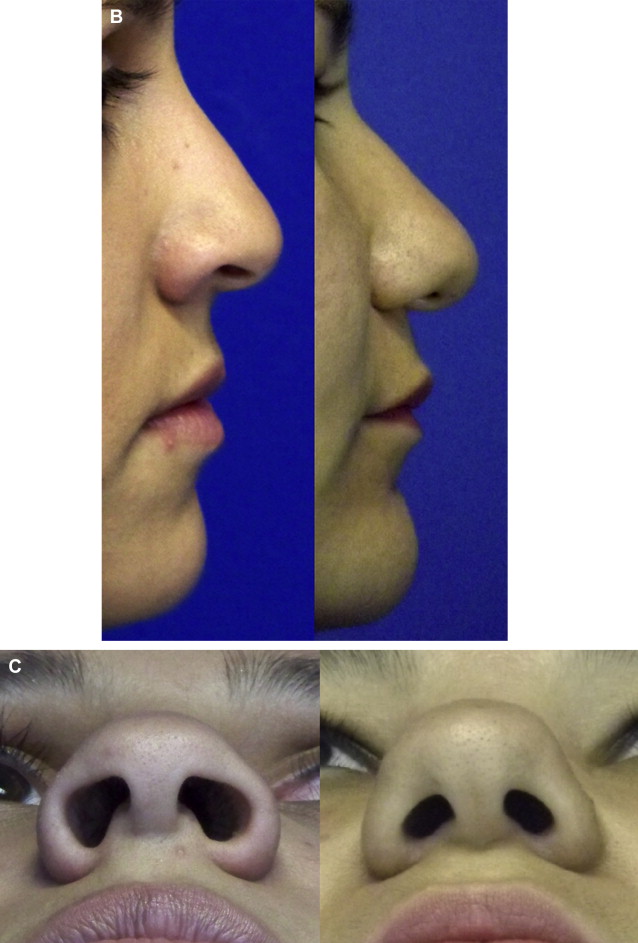
Mestizo nasal and facial characteristics vary frequently because much depends on which of the different races predominate in the patient’s features. In general, the Mestizo nose could be classified as having messorhine characteristics ( Table 1 ). The underlying cartilaginous and bony framework is frequently weak with a covering (skin–soft tissue envelope [S-STE]) that tends to be thick, resulting in an external appearance that shows a nose that is bulbous and undefined and can look slightly flattened ( Fig. 2 ). Mestizo patients are also known as “Hispanics” and “Latinos” and the 3 terms can sometimes be used interchangeably, although the term Mestizo is the one that most closely defines racial features.
| Nasal Characteristics | Mestizo Patients |
|---|---|
| Skin type | Normal/thick/sebaceous |
| S-STE | Thick/tendency toward inflammation |
| Nasal bones | Normal to short |
| Bony dorsum | Normal to low radix Wide nasal bridge Small pseudohump |
| Cartilaginous nasal vault | Normal to weak, wide |
| Nasal tip/alar cartilages | Flimsy/unsupportive/wide/undefined Poor tip recoil |
| Columella | Normal to short |
| Nasolabial angle | Normal to acute |
| Nasal spine | Normal to short |
| Nostril shape | Horizontal shape/sometimes flaring |
| Alar base | Normal to wide |

Definition of problems/planning the surgery
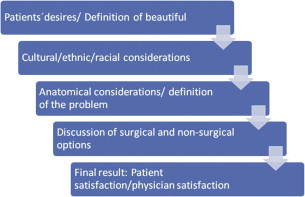
A stepwise approach is usually used when planning a rhinoplasty procedure ( Fig. 3 ).
- 1.
Patient’s desires/definition on what is beautiful to patient
The big question when performing Mestizo rhinoplasty is, what do patients want? In the author’s experience, Mestizo patients want smaller noses with more defined-looking features.
- 2.
Cultural/ethnic/racial variations
Latin American Mestizos do not have a specific racial pattern. Individual facial and nasal features will be defined on particular migration patterns of the geographic area from where the patient is coming from. Today, Mestizo patients are considered mixed race patients wherein a blending of characteristics is what can be found as a predominant facial feature.
- 3.
Physical examination/anatomic diagnosis/definition of problems
An accurate physical examination to try to make a correct diagnosis of the different anatomic structures of the nose will let the surgeon establish in an efficient way the different findings of the nose. In this way, a precise definition of the different problems can be established to be able to define what type of solutions can be offered.
- 4.
Photographic documentation
Six standard rhinoplasty views are routinely taken on all patients: front view, base view, left lateral view, left oblique view, right lateral view, right oblique view. These images are used to perform computer imaging with the patient where possible cosmetic results are shown to try and define if they fit with the patient’s desires of what he or she wants with their nose. When working with computer imaging, it is very important to show patients realistic images of the changes that can be obtained. Preoperative images are used during surgery and they become an integral part of the patient’s medical record. They are constantly used during postoperative visits to show patients how their results are evolving. Postoperative pictures are again taken at 6 months and 1 year after surgery and if possible every year thereafter. This systematic documentation helps evaluate long-term results and aids the surgeon in evaluating surgical techniques used.
- 5.
Discussion of surgical and nonsurgical options
Depending on the patient’s physical findings, possible surgical options must be discussed and clarified. It is important for patients to understand the limitations and the existing risks of the surgical procedure that is being offered. The final result ideally should be a patient who is happy with his final result and a surgeon who is happy with the type of surgery he performed and the result obtained.
As mentioned above, patients usually want noses that look smaller and more defined. Anatomically, surgeons are frequently faced with noses that have very poor underlying cartilaginous and bony support structures and a thick S-STE. Surgery should be oriented toward reinforcing support structures of the nose and creating definition of nasal dorsum and tip without resulting in a nose that looks big or bulky.
Structural approach in the Mestizo nose
When performing rhinoplasty in Mestizo patients, the author has used a structural approach for more than 20 years to tailor the surgery depending on the patient’s individual needs. All procedures are done under general anesthesia and generally an open approach is used. The philosophy behind this structural approach is as follows:
- •
Conservative tissue excision
- •
Preservation and reinforcement of support structures of the nose
- •
Structural grafting to reinforce and increase strength of existing anatomic structures
- •
Precision grafting and filling and exact suture placement to define nasal structures
To help plan the surgery accordingly, the nose is divided into anatomic thirds. Specific techniques are planned for each area and cartilage grafting is planned depending on the needs of each individual patient.
- •
Upper third of the nose (bony dorsum)
- •
Middle third of the nose (cartilaginous dorsum)
- •
Lower third of the nose (nasal tip)
The upper and middle third of the nose (including osteotomies) are usually managed before final tip procedures are performed ( Tables 2 and 3 ).
| Problem | Surgical Solution |
|---|---|
| Wide dorsum no hump | Medial and lateral osteotomies |
| Low radix/small pseudohump | Radix graft |
| Low dorsum | Dorsal augmentation |
| Weak ULC | Spreader grafts Mattress flaring sutures Onlay grafts |
| Anatomic Problem | Surgical Solution |
|---|---|
| Intact strip procedures | |
| Wide alar cartilage | Cephalic trim of lateral crura Lateral crural turn in flap |
| Suture defining techniques | Lateral crural steal Dome-defining sutures Lateral crural spanning sutures Septocolumellar suture |
| Incomplete strip procedures | |
| Overprojected tip/long plunging nose | Lateral crural overlay technique Medial crural overlay technique |
| Grafts on the nasal tip | |
| Grafts that increase support and create definition | Shield graft Lateral crural strut graft Alar rim grafts Morcelized cartilage over nasal tip |
Surgical technique
All surgeries are done under general anesthesia. The nose is infiltrated using 1% to 2% Xilocaine + epinephrine 1:100,000.
Harvesting of Cartilage
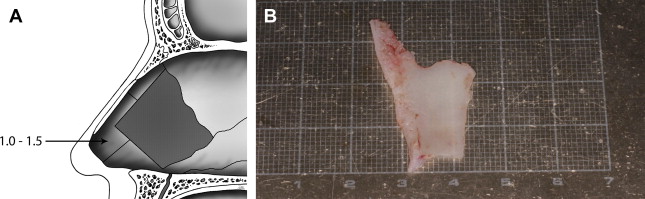
The first choice for cartilage grafting is the nasal septum. In Mestizo patients, because of the mesorrhine configuration of their nose, the quadrangular cartilage is not very big and is usually not thicker than 2 to 3 mm. This small amount of cartilage is a big limitation because the amount of cartilage available for grafting can sometimes be limited. It becomes imperative to harvest the cartilage as a complete block, leaving at least 1.5 cm caudally and dorsally and leaving a complete inverted L of septum in the nose that will be an important support after surgery. Access to the nasal septum can be gained using a Killian or a caudal septal incision. All deviations are straightened as much as possible, especially those present caudally. The septum is closed using a continuous mattress absorbable suture ( Fig. 4 ).
The Open Approach
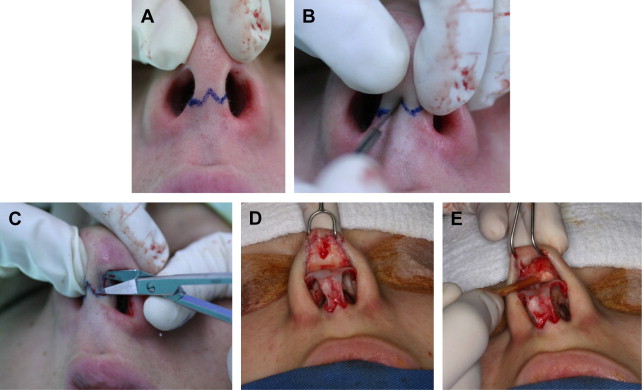
An inverted V incision is placed at the mid-columellar region immediately above the feet of the medial crura and extending laterally 2 mm behind the crura. Cuts are done perpendicular to the skin, using a no. 15 blade. Laterally, the incision is extended superiorly following the caudal of the intermediate crura and lateral crura.
The flap is elevated using converse scissors, keeping the dissection plane below the musculoaponeurotic system and immediately above the cartilaginous structures of the nasal tip. Once the nasal tip has been dissected, the dissection moves to the midline, elevating the skin over the cartilaginous middle third of the nose, directly over the perichondrium, and after the nasal bones are identified, the dissection is done subperiosteally all the way up to the nasofrontal angle ( Fig. 5 ).
The Upper Third of the Nose (Bony Dorsum)
In Mestizo patients, nasal bones tend to be short and somewhat flattened. Anatomically common findings are as follows:
- a.
Wide nasal dorsum without hump
- •
Surgical technique: medial and lateral osteotomies
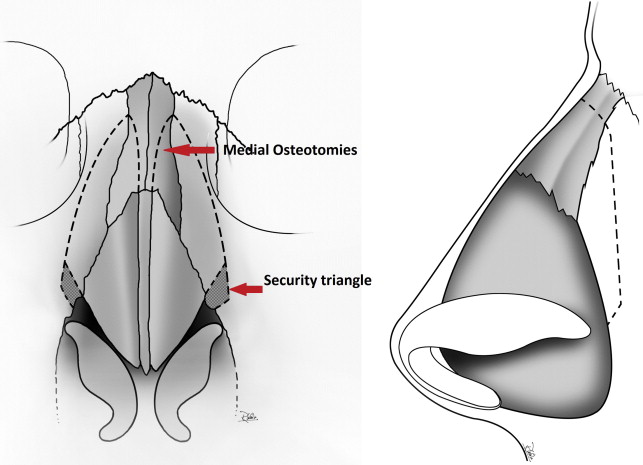
Medial and lateral osteotomies will help narrow a wide dorsum without changing the dorsal height. Medial osteotomies are done first using a 3- to 4-mm curved osteotome. The osteotomy is started in the midline at the junction of the dorsal edge of the septum and the bony dorsum. The osteotome is angled 20 to 30° off the midline to avoid the thick frontal bone. Lateral osteotomies are performed using a 2.2-mm guarded osteotome using a high-low-high technique ( Fig. 6 ).
- •