For Asian people with poorly developed dorsal height and tip height combined with thick skin, augmentation is the most common procedure in rhinoplasty. Nasal deformities are also prevalent. Frequent use of dorsal augmentation material and grafting procedures in Asian rhinoplasty results in a relatively high rate of revision surgery to correct complications. This article describes dorsal augmentation using alloplastic implant materials and several tip grafting procedures. Surgical techniques for the correction of a deviated nose and convex dorsum are also discussed, with emphasis on extracorporeal septoplasty as modified by the senior author. A technical guide is described to treat this condition.
Key points
- •
In augmentation rhinoplasty for Asian people, tip surgery using autologous cartilage followed by dorsal augmentation using alloplastic implant materials such as Gore-Tex (expanded polytetrafluoroethylene) or silicone is the most commonly performed procedure.
- •
Tip grafting procedures including shield grafting, multilayer tip grafting, and modified vertical dome division are mainstays in improving the Asian nasal tip.
- •
For severely deviated Asian noses, the senior author’s modified extracorporeal septoplasty technique is useful before augmentation.
- •
A short-nose deformity is one of the typical problems in revision surgery for Asian people and requires the surgeon’s best effort in correcting, using various maneuvers such as the use of extended spreader grafts and dorsal augmentation.
- •
Costal cartilage is an important graft material for Asian rhinoplasty; however, it is best reserved for primary surgery in thick-skinned individuals with poorly developed noses and complicated revisions.
Anatomic characteristics of the Asian nose
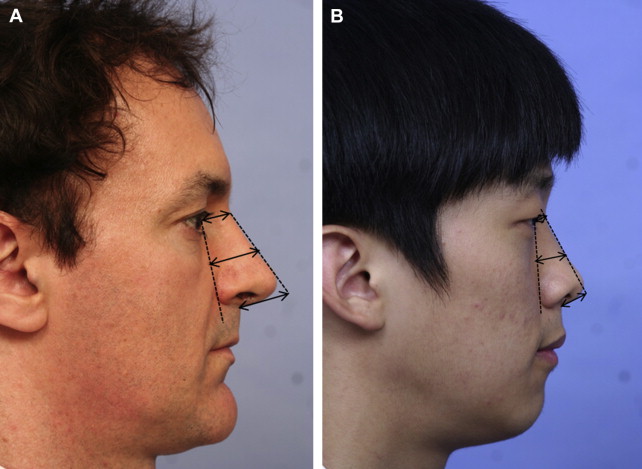
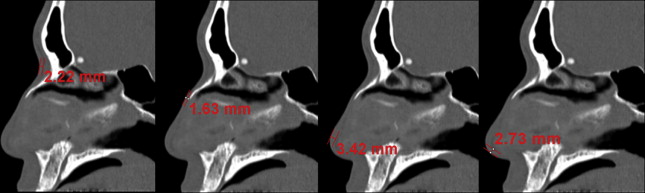
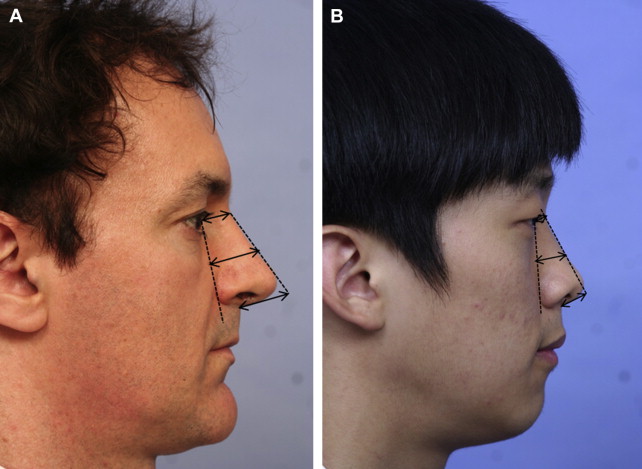
The tip of the Asian nose, particularly the east Asian or oriental nose, is usually low, and the lower lateral cartilages are small and weak. The nasal bones are flat and thick, resulting in a low radix. The average nasal length/nasal tip projection/dorsal height/radix height ratio of the nose in white people has been shown to be 2:1:1:0.75 ( Fig. 1 A). However, in the senior author’s study, young Koreans had a nasal length/nasal tip projection/dorsal height/radix height ratio of 2:0.97:0.61:0.28 (see Fig. 1 B). This finding supports the popularity of augmentation rhinoplasty to correct a low-profile nose among Asian people. Regarding the septum, the septal cartilage of some Asian people is thin and small. In a study of the senior author’s patients having external rhinoplasty, intraoperative measurement of the harvested septal cartilage was performed with preservation of L struts 10 mm wide. The mean caudal length of the harvested septal cartilage was 15.1 mm, and the mean dorsal length was 18.2 mm. Therefore, the size and the quantity of harvestable septal cartilage may be inadequate for complex rhinoplasty procedures, increasing the need of harvesting grafts from other sites. Typical Asian noses tend to have thicker skin than noses of white people, with abundant subcutaneous soft tissue. In the senior author’s research using computed tomography (CT) scans of the nose of Koreans, the mean nasal skin thickness was 3.3 mm at the nasion, 2.4 mm at the rhinion, 2.9 mm for the nasal tip, and 2.3 mm for the columella ( Fig. 2 ). In this study, the thick skin at the nasal tip and columella was associated with poorer surgical outcomes, suggesting that regional skin thickness is an important prognostic factor for tip surgery success.
Anatomic characteristics of the Asian nose
The tip of the Asian nose, particularly the east Asian or oriental nose, is usually low, and the lower lateral cartilages are small and weak. The nasal bones are flat and thick, resulting in a low radix. The average nasal length/nasal tip projection/dorsal height/radix height ratio of the nose in white people has been shown to be 2:1:1:0.75 ( Fig. 1 A). However, in the senior author’s study, young Koreans had a nasal length/nasal tip projection/dorsal height/radix height ratio of 2:0.97:0.61:0.28 (see Fig. 1 B). This finding supports the popularity of augmentation rhinoplasty to correct a low-profile nose among Asian people. Regarding the septum, the septal cartilage of some Asian people is thin and small. In a study of the senior author’s patients having external rhinoplasty, intraoperative measurement of the harvested septal cartilage was performed with preservation of L struts 10 mm wide. The mean caudal length of the harvested septal cartilage was 15.1 mm, and the mean dorsal length was 18.2 mm. Therefore, the size and the quantity of harvestable septal cartilage may be inadequate for complex rhinoplasty procedures, increasing the need of harvesting grafts from other sites. Typical Asian noses tend to have thicker skin than noses of white people, with abundant subcutaneous soft tissue. In the senior author’s research using computed tomography (CT) scans of the nose of Koreans, the mean nasal skin thickness was 3.3 mm at the nasion, 2.4 mm at the rhinion, 2.9 mm for the nasal tip, and 2.3 mm for the columella ( Fig. 2 ). In this study, the thick skin at the nasal tip and columella was associated with poorer surgical outcomes, suggesting that regional skin thickness is an important prognostic factor for tip surgery success.
Augmentation rhinoplasty
The purpose of this procedure is the cosmetic improvement of typical low-profile noses without deviation, saddle or hump deformities, or a short-nose deformity.
Dorsal Augmentation
Dorsal augmentation is the most commonly performed procedure in Asian rhinoplasty. It is also critically important not only in simple cosmetic rhinoplasty but in all types of rhinoplasties in order to achieve aesthetic perfection. Unlike the rhinoplasty for white people, in Asian rhinoplasty, alloplastic implants still play an important role because of the differing anatomic characteristics of Asian noses, such as thick skin and poorly developed cartilaginous framework. There is no single ideal implant or graft for dorsal augmentation. Every material has its own merits and drawbacks. Aesthetic perfection of the nose is determined by the height and shape of the nasal dorsum seen from the side and front, with its harmonious alignment with the nasal tip. The dorsal implant should be designed with the appropriate width, and the thickness of the patient’s skin must be taken into consideration. In patients with thin skin, it is preferable to use soft implants such as expanded polytetrafluoroethylene (ePTFE) rather than silicone. In patients with thick skin, a more solid material such as silicone, reinforced ePTFE, or costal cartilage can be used without causing significant problems. In the senior author’s experience, it is easier to get favorable aesthetic outcomes of dorsal augmentation when alloplastic implants are used, compared with the use of biological implants including autologous and homologous cartilage and fascia. Long-term follow-up of patients having rhinoplasty shows that aesthetic complications are more frequent in biological implants. These complications included visibility of the dorsal cartilage implant, warping, absorption, or deformation. Infections immediately following surgery are more common in biological implants, whereas delayed inflammations and infections are more common in alloplastic implants and if not treated adequately, can cause serious deformities.
Alloplastic implants
ePTFE and silicone are the most widely used alloplastic implants in Asian rhinoplasty ( Fig. 3 ). ePTFE implants have microscopic pores that induce the surrounding tissue to grow into them, thus having the advantages of increased stability and lower incidence of capsule formation. In addition, the risk of extrusion is lower with ePTFE than with silicone. The soft texture of ePTFE reduces patient discomfort, and implant visibility through the skin is less common than with silicone implants. ePTFE is available in different thicknesses. If a surgeon uses a sheet-type ePTFE implant of 1-mm to 2-mm thickness, multiple sheets should be stacked to get a sufficient increase in dorsal height. The advantage of using sheet implants is that augmentation levels can be adjusted for each region easily, even for patients with focal prominence or depression in the dorsum ( Fig. 4 ). When using ePTFE, sufficient beveling of the sheet’s margins is essential, especially for sheets of more than 2-mm thickness. If not beveled correctly, the implant’s margins can be felt through the skin after surgery. One notable disadvantage of ePTFE is that it decreases in volume after insertion. In addition, it is more difficult to remove an ePTFE implant from the nasal dorsum than a silicone implant. Delayed inflammation is serious complication in the use of this material. It has been reported that the infection rate in primary surgery is 1.3%, whereas in secondary surgery it is 4.3% to 5.4%.
Prefabricated silicone implants are the most popular material in dorsal augmentation for Asian noses. Because of its stable chemical structure, silicone has several advantages, including its low tissue reaction and ease of handling. Moreover, the availability of ready-made products makes implantation convenient, and the relative hardness of silicone makes it suitable for fashioning the desired nasal shape for Asian people with a moderately thick to thick skin. Placement of an I-shaped implant at the nasal dorsum with tip plasty using autologous material (septal or conchal cartilage) is the preferred surgical method. When inserting silicone implants, the caudal end of the silicone implant should not be in direct contact with the tip skin. The caudal end of the implant is usually located in the space between anterior septal angle and alar cartilages, connecting the nasal dorsum with the nasal tip. Placement of stacked tip onlay grafts on the dome area, which is in direct contact with the tip skin, is frequently performed with silicone implantation ( Fig. 5 ). Revision rhinoplasty after silicone implantation may be needed for implant deviation, floating, displacement, extrusion, impending extrusion, infection, and contraction of skin resulting in a short-nose deformity.
Autologous cartilage
Autologous materials are advantageous for dorsal augmentation of the nose because these implants are well tolerated and carry the least risk of infection. However, there is the issue of donor site morbidity. In addition, the aesthetic performance of these materials is generally worse than alloplastic implants, at least with respect to dorsal augmentation. Common autologous tissues used for dorsal augmentation include septal cartilage, conchal cartilage, costal cartilage, fascia, and dermofat.
Because it is easy to harvest and shape the septal cartilage, septal cartilage can be used to moderately elevate the nasal dorsum, to camouflage a partial concavity on the dorsum, and for nasal tip surgery. However, the use of septal cartilage for dorsal augmentation is impractical in 1-piece dorsal augmentation of the noses of Asian people. First, it is difficult to obtain a long enough piece of cartilage (3–4 cm) for dorsal augmentation because the septal cartilage harvested is small. Second, using cartilage for cosmetic dorsal augmentation is less aesthetically pleasing compared with alloplastic implants because it is difficult to carve the cartilage as smoothly as alloplastic implants.
Conchal cartilage, unlike septal cartilage, has an intrinsic curvature that complicates its routine use in dorsal augmentation. In addition, the conchal cartilage is frequently too small to yield a cartilage piece suitable for 1-piece dorsal augmentation. A method avoid this problem is the use of diced conchal cartilage wrapped with fascia, and this has gained wide acceptance as an ideal dorsal augmentation technique. However, conchal cartilage is preferred in tip surgery, but it is considered to be less suitable as dorsal augmentation material.
Although costal cartilage is difficult to harvest and is associated with serious donor site morbidities such as pneumothorax, as well as the problem of implant warping, it is the most useful autologous cartilage for thick-skinned primary cases, which require substantial augmentation, or in patients who have experienced complications with alloplastic implants ( Figs. 6 and 7 ).





