Rhinoplasty in patients of African descent requires a patient-specific approach, because the goals and ideal proportions differ from the white nose. This article discusses approaches to surgical correction of common anatomic variations. In addition, common pitfalls are outlined.
Key points
- •
There is significant variation in nasal anatomy among patients of African descent.
- •
The goal of surgery is to address only what the patient requests as change to their nose and not to duplicate a preconceived nasal ideal.
- •
Balance dorsal augmentation with tip projection.
- •
Avoid excessive alar base narrowing because it can create deformity and disharmony.
- •
Creating aesthetic refinement while maintaining ethnic features is key to successful surgery.
Introduction
As the ethnic demographics of the nation continue to evolve so too does the demand for facial plastic surgery among patients of diverse ethnic backgrounds. Today’s surgeon must approach each patient as a unique individual with a distinct set of goals for that patient. Patients of African descent who seek out rhinoplasty surgery have similar motives as those of other groups seeking rhinoplasty surgery: to improve nasal aesthetic harmony and nasal function, and not for racial transformation.
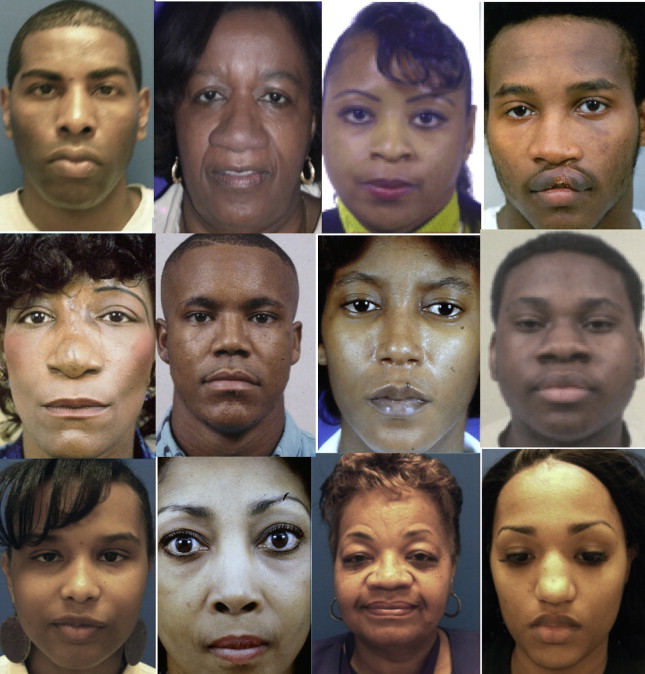
In 1976, the senior author published an article concerning the nonwhite rhinoplasty. At that time, there was little in the literature concerning the subject and it was a rare surgeon with significant expertise in this area. Before that time there had been many generalizations and misconceptions reported on the nasal anatomy of those of African descent, and this article advocated for the recognition that most patients do not exhibit all of those anatomic features ( Fig. 1 ) and that the goal of each rhinoplasty should be to create harmony in an individual and not to duplicate a preconceived nasal ideal. Since that time, many others have expanded on this conversation and the practice of patient-specific surgery has gained almost universal acceptance.
Now, almost 40 years later, the number of patients of African descent has increased as has the number of facial plastic surgeons who routinely manage these patients. Recent surveys on plastic surgery trends have reported that African Americans constitute 7% to 8% of all plastic surgery patients. According to the 2012 American Academy of Facial Plastic Surgery 2012 survey, 27% of surgeons report an increase in African American patients seeking facial plastic surgery and 80% of these patients are seeking rhinoplasty.
Introduction
As the ethnic demographics of the nation continue to evolve so too does the demand for facial plastic surgery among patients of diverse ethnic backgrounds. Today’s surgeon must approach each patient as a unique individual with a distinct set of goals for that patient. Patients of African descent who seek out rhinoplasty surgery have similar motives as those of other groups seeking rhinoplasty surgery: to improve nasal aesthetic harmony and nasal function, and not for racial transformation.
In 1976, the senior author published an article concerning the nonwhite rhinoplasty. At that time, there was little in the literature concerning the subject and it was a rare surgeon with significant expertise in this area. Before that time there had been many generalizations and misconceptions reported on the nasal anatomy of those of African descent, and this article advocated for the recognition that most patients do not exhibit all of those anatomic features ( Fig. 1 ) and that the goal of each rhinoplasty should be to create harmony in an individual and not to duplicate a preconceived nasal ideal. Since that time, many others have expanded on this conversation and the practice of patient-specific surgery has gained almost universal acceptance.
Now, almost 40 years later, the number of patients of African descent has increased as has the number of facial plastic surgeons who routinely manage these patients. Recent surveys on plastic surgery trends have reported that African Americans constitute 7% to 8% of all plastic surgery patients. According to the 2012 American Academy of Facial Plastic Surgery 2012 survey, 27% of surgeons report an increase in African American patients seeking facial plastic surgery and 80% of these patients are seeking rhinoplasty.
Preoperative consultation
Unfortunately, insensitivity to a patient’s ethnic features, and the well-known disastrous rhinoplasty results of certain celebrities, have created some suspicion and caution among many African American patients. Therefore, it is important to recognize and address any trepidation and misconception in the preoperative visit. Even patients presenting with a nasal bone fracture or a deviated nasal septum often voice concerns about changes to the appearance of their nose. This is the opportunity to establish the necessary rapport with the patient and to let them know that you share their concerns and are sensitive their specific requests for nasal modifications.
The patient should be asked to identify those specific areas that they would like changed. This may be difficult for the patient to express precisely and often it is helpful to use a mirror and have them point out the regions of their nose that they wish to be addressed. Some modifications can even be manually simulated and computer imaging may be of further assistance. Often the patient states that they just want their nose to “look better.” Approach these patients with caution, because their vision of a “better” nose may be incongruous to yours.
At this time, it is appropriate to then point out some of the common anatomic findings in a nose of African descent. You can then balance your nasal analysis with the patient’s requests. Be sure to share your findings with the patient. As white surgeons, the authors also find that it is helpful to compare our own noses with the patient’s and to point out the differences between the two. Let the patient know that you recognize that everyone’s nose need not appear the same, and this often can help allay their concerns and open a dialogue on creating facial harmony.
Although many of our African American patients have similar goals of nasal modification as patients of any other descent (eg, correction of crooked nasal deformity, internal valve collapse, tip ptosis), there are certain requests that are common to this patient population. In their survey of 196 patients, Baker and Krause found that most patients did not want their modifications to resemble white noses and that the most common complaints were that their noses were “too large, too broad, or too wide.” Momoh and colleagues report that patients of African descent commonly wish to address specific features: “alar flare, tip definition, dorsal irregularities, and decreased tip projection.” Rohrich and Muzaffar describe the goals of African American rhinoplasty to be “maintaining nasal-facial harmony and balance; a narrower, straight dorsum; enhanced tip projection and definition; slight alar flaring; and narrower interalar distance.”
Not all patients desire all of these stated goals, nor are they realistically obtainable. For example, many patients only want more tip definition and not a change in their interalar distance. It is important to address only the patient’s goals and not the generalized goals of the surgeon. However, even if the patient wants some of these changes addressed, they often do not want these changes taken to the extreme of conforming to a European nasal ideal.
Another concern in the preoperative consultation is the patient who presents desiring radical changes to remove their features that suggest an African heritage. We recommend avoiding surgery in these patients. In the future we may see more patients requesting rhinoplasty to accentuate, and not to hide, their African heritage.
Failure of a patient to clearly identify the changes they wish or a surgeon’s failure to realistically appreciate what the patient wants, or whether he or she can realistically achieve those goals, should be absolute indicators not to proceed with surgery. This mature approach often results in these issues being resolved.
General anatomic concerns
It must be reiterated that patients of African descent do not all share the same nasal anatomy, because there is significant variability among this patient population depending on their own individual heritages. However, there are some general anatomic features that are consistently seen.
The skin is typically thick with an abundance of subcutaneous fibrofatty tissue. This layer often measures between 2 and 4 mm in thickness. This thick soft tissue envelope is especially noticeable in the nasal tip in which the thick skin contributes to the creation of a broad and bulbous appearance. This thickened skin makes it more difficult to see and feel the shape of the lower lateral cartilages (LLCs) through the skin during the preoperative assessment. It is surgically more difficult to create noticeable changes and refinement in the nasal tip.
The size and strength of the LLCs also contribute the wider appearance of the tip. The LLCs in patients of African descent have often been described as being somewhat shorter in total length and more flaccid. However, in a cadaver study conducted by Ofodile and James, the average width and height of the LLCs were reported to be similar in size to that of white noses. However, their study only focused on measurements of the lateral crus. It is likely that a widened alar base gives the appearance of shortened lateral crura in relation to the overall width of the nose. The relationship of the medial crura (which is also thought to be shorter in general) to the lateral crura is more likely responsible for the broad nasal tips commonly seen in patients of African descent. The intradomal angle is often described as large and obtuse, which can lack the sharp, acute definition of the intermediate crus seen in the white nose. The nasal spine is also less prominent, which translates to even less tip projection. The angle of inclination of the LLCs in relation to the plane of the maxilla may also be more acute and cause an underrotation of the tip. In patients of African descent, Ofodile and Bokhari reported the average nasolabial angle to be 91 degrees in women and 84 degrees in men ( Fig. 2 ). Contrast these figures to the ideal nasolabial angles ranging from 90 to 105 degrees recommended by most surgeons.
The underlying bony structure also differs. The pyriform aperature is described as wider and more oval in shape. This spreads the base of the nose more lateral, increasing the interalar distance and decreasing nasal projection. Based on anthropometric measurements, Porter found the ratio of intercanthal distance to nasal width to be 1:1.3 in African American men compared with the classically described 1:1 relationship based on the white nose. Excessive alar flare, such that the edge of the ala extends greater than 2 mm lateral to the alar base attachment, is also commonly seen. The shape of the nostrils varies but can often approximate a horizontal orientation. This horizontal orientation moves the classical 2:1 columella to lobule ratio to closer to a 1:1 ratio ( Fig. 3 ).
Short nasal bones are commonly encountered. In combination with the widened pyriform aperture and decreased height of the ascending maxilla, these shortened nasal bones create a low and broad nasal dorsum. Therefore, the nasofrontal angle is often more obtuse, 127 to 133 degrees, in comparison with 120 degrees in the white nose. These shortened nasal bones and low dorsum may contribute to the authors’ observation that nasal bone fractures in patients of African descent often do not result in the visible asymmetries commonly requiring correction in the white nose. There is no doubt that nasal fractures and the subsequent deformities are less common when compared with a comparable white population. Unfortunately, this results in more subtle deformities and often delayed and/or underrecognized abnormalities.
This broad, lowered dorsum also translates down into the upper lateral cartilages, which can result in a broad middle third. These differences may impact nasal function in some patients. As the height of the internal valve is lowered, the shape of the surface area for nasal airflow is placed more inferiorly and centered more on the head of the inferior turbinate. Thus, the inferior turbinates have a more significant role in nasal obstructive symptoms in patients with this nasal anatomy.
Surgical techniques
Whether to use an endonasal technique or perform an external approach is essentially dictated by the changes sought, the preference of the surgeon, and the patient’s concerns. Another important consideration is the potential for surgical change in the individual patient. Some preoperative maneuvers answer these questions ( Fig. 4 ). The authors’ personal philosophy for all nasal surgery is to use the least complex technique that permits accomplishing the desired changes. Many surgeons prefer to use an external approach in patients of African descent. We also find that the increased exposure afforded by the external approach allows for creation of the more dramatic changes that are often necessary in the nose of patients of African descent. However, routine tip surgery can still be accomplished by way of an endonasal approach. The placement of a columellar strut, which is one of the most common maneuvers used in these patients, can easily be placed by way of an endonasal technique ( Fig. 5 ). As a general rule, if a tip graft is contemplated, then an external approach with a transcolumellar incision is used.





