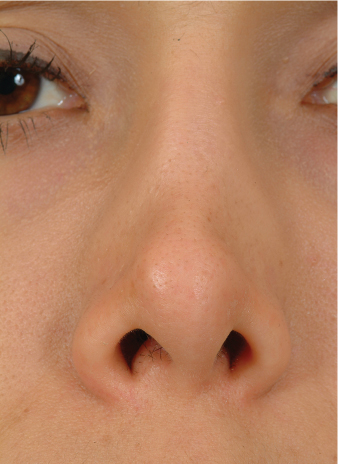
10 Most plastic surgeons consider rhinoplasty one of the most complex facial plastic operations. Precise preoperative diagnosis and meticulous surgical technique are required to produce a favorable outcome and avoid complications. As anatomies differ and patient expectations vary, no single technique is appropriate for all patients. Rhinoplasty complications not only encompass those common to most surgeries, such as infection and hematoma, but also are frequently associated with functional and aesthetic problems. Traditional rhinoplasty techniques involve reductive, excisional methods, which may be associated with many untoward long-term changes. Grafting in rhinoplasty may also result in problems, such as graft visibility, mobilization, and extrusion. Methods to prevent or correct common rhinoplasty complications are detailed below. The preoperative consultation is a critical step to avoid complications after rhinoplasty. It is essential that both the surgeon and patient have realistic expectations. If they cannot achieve common goals, due to either patient limitations (e.g., damaged soft-tissue skin envelope) or a surgeon’s inexperience with or lack of comfort in performing the proposed procedure, the surgery should not proceed. This is especially true in patients seeking secondary rhinoplasty. Computer imaging of the proposed changes can facilitate communication between the surgeon and patient. Perhaps more importantly, it can also provide a visual explanation of the proposed outcome. Patients often have difficulty expressing the changes they desire, or they may be unaware of what results are realistic and surgically attainable. Computer imaging may help overcome this problem. In fact, one study demonstrated that patient satisfaction was significantly improved when the procedure included preoperative imaging versus no imaging.1 If computer imaging is used, the image shown should realistically represent what the surgeon can achieve. In fact, under-imaging, or showing less than ideal outcomes that the surgeon can generally achieve, is the most effective means of using computer imaging. The surgeon is warned against trying to sell the operation with unrealistic or idealized imaging. The surgeon must assess the quality and thickness of the skin/soft tissue envelope (SSTE) preoperatively. In fact, a damaged SSTE may be the deciding factor as to whether or not a revision rhinoplasty can be undertaken. In some cases, significant scar tissue may be present from a previous surgery in which aggressive thinning of the subcutaneous tissue and/or dissection in the incorrect plane took place. If patients have an immobile SSTE that adheres tightly to the underlying cartilaginous framework, surgery is postponed until the SSTE loosens. In cases of severely damaged SSTE, surgery may not be offered at all. At times, the SSTE will be thin or devascularized from prior surgery. Visible irregularities, cutaneous telangiectasias, and purple discoloration of the skin are signs of SSTE damage (Fig. 10.1). It is important that these skin changes are recognized, because in such cases extensive soft-tissue elevation may lead to ischemia and skin necrosis. Moreover, revision surgery should be postponed until changes in skin color resolve, which may take years. Any irregularities or skin damage should documented in the chart and by close-up photography before surgery. Finally, the patient with a damaged SSTE needs to be counseled preoperatively about the risk of further skin damage, even necrosis, with surgery.2 During the preoperative evaluation for secondary rhinoplasty, the surgeon should assess the patient for the presence of alloplastic implants. These implants may result in SSTE damage and significant scar tissue (Fig. 10.2). The surgeon should be prepared to replace the alloplastic implants with alternative grafting materials, such as cartilage. The surgeon should discuss the postoperative healing process candidly at the initial consultation. The patient should be aware that postoperative nasal edema is normal in the healing period and may be significant, especially in patients with thick skin. Patients should be made aware that the healing process will continue throughout their lifetime as wound contracture continues; therefore, aesthetic changes will occur over a period of many years. Risks and possible complications should also be discussed. Fig. 10.1 Patient who underwent previous rhinoplasty with excessive thinning of the supratip skin that resulted in permanent damage. Fig. 10.2 Patient with an infected MEDPOR dorsal implant. The dorsal skin is severely damaged and scarred from the infection. Treatment required removal of the implant and resolution of the infection prior to reconstruction. A thorough medical history should be taken, and physical examination should be performed. All prior nasal surgery should be documented, and any accessible reports of these operations should be reviewed. Pre-operative laboratory and other diagnostic studies need to be obtained. The specific panel of studies ordered is chosen according to the patient’s age and overall health. A complete blood count and coagulation studies are performed on every patient. Any history of unusual bleeding or excessive bruising, as well as any family history of abnormal bleeding, should lead to further investigation. This may involve coagulation studies or a more extensive hematologic workup. In fact, one study found that 9 of 1000 (0.9%) plastic surgery patients were diagnosed with von Willebrand’s disease.3 Patients should also be told to stop aspirin, ibuprofen, vitamin E, and herbal supplements at least three weeks before surgery to reduce the risk of excessive perioperative bleeding. In summary, a careful preoperative evaluation and good communication with a potential rhinoplasty patient may help to avoid some unwanted surgical complications. Unfortunately, many intraoperative errors made in rhinoplasty are either unrecognized or not revealed until the postoperative time period. Therefore, the surgeon must be meticulous to avoid untoward complications. A few specific problems that the surgeon may encounter intraoperatively are described below. As the face is so well vascularized, bleeding is to be expected during rhinoplasty. Excessive bleeding can impair visibility and the surgeon’s ability to execute the desired maneuvers. The use of a topical vasoconstrictive agent and deliberate injection of a local anesthetic containing epinephrine can help to reduce the amount of bleeding. Dissection in the correct plane (just superficial to the perichondrium) can also decrease the degree of bleeding. Bipolar electrocautery is used for hemostasis and should be specifically targeted to reduce the risk of vascular compromise to the SSTE. During dissection, damage to the SSTE or the underlying cartilaginous structural framework may occur. It is preferable to avoid such complications (by careful dissection in the correct tissue plane), but once such problems are encountered, the surgeon must try to correct them. Violation of the SSTE should be treated either by local wound care or (if large) suture reapproximation. If the surgeon recognizes that he is dissecting too superficially (potentially damaging the SSTE), then he should return to the correct tissue plane, take care not to apply a tight nasal dorsal dressing (to avoid compromising the vascular supply to the skin), and monitor the skin closely postoperatively for any signs of damage or necrosis. Another intraoperative complication that warrants discussion is the inadvertent disarticulation of the cartilaginous septal strut from the perpendicular plate of the septum. When this occurs, the strut must be reattached to prevent postoperative saddling. One method of stabilizing the septal strut is to suture it to the nasal bones via holes that are made along the caudal aspect of each nasal bone. Destabilization of the caudal aspect of the septal strut can also occur, which can be repaired by securing the caudal septum to the nasal spine (or its periosteum) with a permanent suture, such as a 5–0 clear nylon suture. Manipulation of the nasal dorsum can lead to middle vault collapse. It is imperative that the surgeon identify preoperatively those patients who may be at risk of middle vault collapse. These include patients with short nasal bones, long weak upper lateral cartilages, thin skin, and a narrow projecting nose (Fig. 10.3).4,5 In patients at high risk for middle vault collapse, several precautions can be taken. Attempts should be made to preserve the middle vault structures, and in many cases augmentation with spreader grafts is recommended. Additionally, osteotomies should be conservative. Preservation of the middle vault mucosa by the formation of precise pockets for spreader grafts will help minimize posterior displacement of the upper lateral cartilages following hump removal.4 Fig. 10.3 Patient with short nasal bones and long upper lateral cartilages. Note the collapse of the upper lateral cartilages, resulting in an inverted-V deformity. One of the more common reasons that patients seek rhinoplasty is correction of a crooked nose. This is one of the most difficult problems encountered in rhinoplasty. Deviated segments of the nose are shifted back to the midline by fracturing bone or manipulating and realigning the cartilage framework. Absolute correction can be difficult to achieve, and there may be residual convexities or concavities along the dorsal nasal subunit that produce contour defects. Ideally, a contour line should be created by shadows that extend from the brow and dorsal nasal subunit to the tip-defining point. Deviation in the upper third of the nose can be addressed with medial or lateral osteotomies. However, inadequate osteotomies may result in a greenstick fracture, which can result in a deviated bony nasal vault postoperatively. In some cases, double lateral osteotomies can be performed to mobilize the bony vault completely and decrease the likelihood of this deformity. However, the surgeon must take care to avoid comminution of the nasal bones, which may lead to their displacement. In many crooked noses, there is also deviation in the lower two-thirds of the nose. It is essential that the cartilaginous structures are reoriented to the midline. If this realignment is not achieved after osteotomies, the nose may shift back to its preoperative position due to the memory of the deviated cartilaginous structures.6 In instances where the nose cannot be shifted back to midline or where a residual concavity exists (as may be seen in a C-shaped deformity), an onlay cartilage graft can be placed lateral to the upper lateral cartilages to camouflage the defect.7,8 A fairly common complication following rhinoplasty is the collapse in the supra-alar region (Fig. 10.4). In patients with a weakened lateral wall, alar batten grafts can be placed prophylactically to prevent the development of any supra-alar pinching. They can also be used to correct preexisting external valve compromise, lateral wall collapse, or supra-alar pinching. An alar batten graft is placed into a precise pocket at the point of maximal lateral wall collapse or supra-alar pinching (Fig. 10.5).9,10 A common tendency is to place the grafts too far cephalically along the upper lateral cartilage, which can result in a persistent fullness in the lateral wall. The surgeon should also avoid dissecting too far laterally, as this may cause bleeding and damage to the lateral nasal arteries that supply the nasal tip. Excessive alar width or flaring may be corrected with alar base reduction. If not done properly, this procedure can lead to significant complications, including unsightly scarring and distorted nostrils (Fig. 10.6). To reduce the risk of visible scars, the skin edges should be everted on closure, which can be achieved by creating a favorable bevel with the excision.11 This bevel should be subtle, with an angle no greater than 10 to 15 degrees. Cautery should be avoided in this area as well, for necrosis or atrophy of the underlying subcutaneous tissue can lead to a depressed scar. Special care should be taken when approximating the subcutaneous tissues to ensure precise alignment. Any time base reduction is performed, conservative removal of tissue is recommended to reduce the risk of nostril distortion or excessive narrowing. Fig. 10.4 Patient with severe supra-alar pinching due to over-resection of the lateral crura. Fig. 10.5 Alar batten grafts can be placed into a pocket at the site of maximal supra-alar pinching. This auricular cartilage graft is placed with its concave surface placed medially. Fig. 10.6 Patient who underwent over-reduction of nasal base, leaving the patient with very small nostrils and airway obstruction. It is critical to avoid visible scars whenever external rhinoplasty is performed. Scarring can be minimized by both careful incisional technique and meticulous closure. Precise reapproximation of the incisions can vastly reduce the visibility of these scars. If the incisions do not align correctly during closure, the surgeon should remove the sutures and try to correct the closure. A subcutaneous suture and multiple 7–0 vertical mattress nylon sutures can be used to close the midcolumellar and alar base reduction incisions. Moreover, careful closure of the mucosal incisions is important to reduce the risk of internal nasal scarring, which can lead to vestibular stenosis and nasal airway compromise. Whenever costal cartilage is harvested for grafting purposes in rhinoplasty, there is a risk of pneumothorax. To ensure that the pleura is intact, the wound cavity is filled with antibiotic solution after the costal cartilage has been taken, and the anesthesiologist creates a positive ventilatory pressure for the patient (a Valsalva maneuver). Air bubbles in the wound should alert the surgeon to a possible rent in the pleura, which should be repaired if identified. The wound is closed over a red rubber catheter placed on suction. With the chest expanded, the catheter can be removed. A postoperative chest X-ray can confirm full expansion of the lungs.
Rhinoplasty Complications
 Preoperative Evaluation
Preoperative Evaluation


 Intraoperative Complications
Intraoperative Complications



Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


