6 Contemporary skin resurfacing procedures—chemoexfoliation, laser resurfacing, and dermabrasion—have been in continual evolution since their inception over 65 years ago and in general represent safe and efficacious techniques for the rejuvenation of aging skin. Like all surgical procedures, resurfacing has associated complications (Table 6.1). Most complications, however, are avoidable if the physician thoroughly understands this family of treatments, including the pharmacokinetics of different wounding agents on various skin types, the histology of depth wounding, normal wound healing, and laser physics. Each modality has a particular mechanism to injure skin and the physician must know how an agent or technique can be used to produce the favorable results desired. By convention, resurfacing procedures are divided by depth of injury into superficial, medium, and deep. The depth of wounding determines the level of destruction and thus the degree of rejuvenation, as well as length of time for wound healing and risk of complications. While superficial wounding will heal within 24 to 48 hours with little risk of problems, medium and deep resurfacing may take considerably longer, and can produce many of the complications to be discussed. In general, resurfacing below the mid-reticular dermis causes destructive necrosis and scarring and should not be performed. Much has been published regarding resurfacing and is available in the literature for physicians to develop a better understanding of its principles and procedures.1,2 When resurfacing devices or peel solutions are overused, inappropriately used, or mismatched with a skin type, unintended injuries and complications may occur.3 Such injuries are the focus of this chapter. Table 6.1 Complications Seen with All Types of Resurfacing
Challenges in Skin Resurfacing
Dyspigmentation |
Scarring |
Infection |
Prolonged erythema or pruritus |
Contact dermatitis |
Textural changes |
Milia |
Acne |
Cold sensitivity |
Worsened doctor-patient relationship |
 Timing of Adverse Events
Timing of Adverse Events
Resurfacing complications can be divided by the timing of their occurrence. Intraoperative problems inadvertently occur during the procedure, and for dermabrasion, an example would be overly aggressive use of the mechanical abrader, creating a wound too deep to heal without a scar. There are documented cases of the wirebrush dermabrader piercing through skin or ripping a lip or eyelid due to lack of surgical control or sudden movement of the patient. One must also be careful not to overuse a freezing agent, which can cause a freeze-burn injury that will create textural scarring or pigmentary alteration.
Intraoperative laser complications include laser-induced fires and laser energy deposition outside the operative field. Proper laser safety precautions should always be mandated, such as keeping wet towel drapes around the operative field and keeping O2 sources and combustible products out of range. The surgeon must give the procedure his full attention so that there are not unwanted laser impacts. Laser-impermeable scleral shields should be used for all facial CO2 or erbium resurfacing cases, especially when performed around the periorbital area. Chemical peel solutions—whether TCA or phenol—are caustic and can cause significant problems if they are inadvertently dripped into the eye or sensitive cutaneous surfaces. The surgeon should personally check the acid and strength before applying and never pass the application over the patient’s central face or eyes. Accidents of this sort have resulted in disastrous corneal damage and cutaneous scars. Over all, however, scarring after all resurfacing procedures—chemical peeling, laser resurfacing, and dermabrasion—has a reported incidence of less than 1%.
Once a resurfacing procedure is completed, the recovery and regrowth of new skin should occur in a controlled environment in which noxious external factors—trauma, allergy, and infection—should be minimized to prevent serious complications. The final common pathway for a resurfacing complication is scarring. This dreaded result can be avoided by careful observation and follow-up during the recovery period, as well as early intervention to reguide the skin to normal healing.4
 Patient Expectations Associated with Resurfacing
Patient Expectations Associated with Resurfacing
The most common risk of skin resurfacing is patient dissatisfaction with the procedure. While it is not a complication in the strictest of terms, many authors view this undesirable outcome as such. This can be avoided by carefully analyzing the patient’s perceived problem and deciding how to realistically treat it with a particular type of procedure.5 It is best to give a patient a mirror and allow them to show you the specific problem that bothers them. Their concern may be fine wrinkles, abnormal color, or inappropriate texture (all effectively treated with erbium laser or medium-depth chemical peeling), or volume defects that require fillers rather than resurfacing. The physician must address the procedure most applicable to achieve the results desired. Repetitive light chemical peels or microdermabrasion can correct pigmentary change but not significant rhytids, which may require a deeper resurfacing procedure. One must then look at patient-specific risks for particular complications, such as hypo- or hyperpigmentation, or the potential for scarring in previously irradiated skin or in the penumbra of a course of isotretinoin.6
It is also important for the physician to distinguish a true complication from an expected side effect of resurfacing and educate the patient appropriately. For example, most ablative resurfacing procedures have expected side effects of transient erythema, flushing, increased skin temperature, pruritus, edema, milia formation, and acne. These are consequences of the new skin formation and should be addressed (as with patient expectations) before the procedure so their appearance will not alarm the patient. Patient reassurance is usually all that is necessary since these problems will resolve spontaneously. Overtreatment of these side effects alone can lead to overtreatment complications.
 Chemoexfoliation: The Workhorse of Resurfacing Procedures
Chemoexfoliation: The Workhorse of Resurfacing Procedures
The most common resurfacing procedure performed under the direction of a physician is chemical peeling. Generally, light chemical peels have fewer complications than any of the others. These peels are “lunch time” procedures designed to exfoliate the upper epidermis with minimal dermal inflammation. Healing is usually uncomplicated, occurring in 1 to 3 days. Untoward problems can occur with overcoating low-dose trichloracetic acid (TCA), leaving glycolic acid in place for prolonged periods without proper neutralization, or over-aggressive degreasing of the skin prior to the peel.7 These can result in edema, prolonged erythema, excessive pain, prolonged exfoliation, and delayed healing. Hyperpigmentation and scarring can occur. Practitioners should be especially concerned with sensitive-skinned patients, such as those with atopy, or patients using regular exfoliating programs or retinoids or other skin-care programs that may thin the stratum corneum. Most of these problems are reversible with skin protection, bland emollients and appropriate treatment, such as topical corticosteroids and bleaching agents. In well-trained hands, unmet expectation is the prime risk associated with light chemical peels.
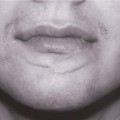
If medium or deep resurfacing is chosen as the procedure to solve a patient’s skin problem, the physician must discuss the patient’s expected down time, temporary side effects such as erythema, pruritus, and skin sensitivity, as well as care instructions for for 7–14 days of healing. Doing so will likely yield a favorable result with a happy patient. Not doing so can produce complications—reversible or irreversible—and an unhappy patient. Medium and deep resurfacing create full-thickness destruction of the epidermis along with partial necrosis and inflammation of varying levels of dermis. With medium depth chemical peeling, aggressive overcoating with 35% of TCA or combination TCA peels can drive a medium peel into a much deeper destructive procedure and potentially cause scarring (Fig. 6.1).7 The most common complication, though, is hyperpigmentation, which can last up to 3 months, depending on skin type and postoperative care. Medium and deep chemical peels along with deep resurfacing procedures, such as CO2 resurfacing or dermabrasion, must be considered more serious surgical procedures and deserve the appropriate preoperative consultation and informed consent with a thorough understanding of the postoperative care and sequelae.
 Dyspigmentation
Dyspigmentation
Alterations in pigmentation after resurfacing procedures can be either desirable or constitute a complication. Desirable pigmentary changes include lightening uneven dyschromias or correcting conditions such as melasma or age-related hyperpigmentation. Unintended pigmentation changes, such as streaks or irregular lines of demarcation, can occur from uneven degreasing, inhomogeneous chemical application, or inappropriate choice of wounding agent. TCA 50%, for example, has fallen out of favor as a resurfacing treatment because of its increased complication profile, including dyspigmentation and scarring. Post-peel pigmentary inhomogeneity typically occurs around the eyes, mouth, or jawline margin adjacent to the untreated neck. Such irregularities are not specific to chemical resurfacing, but also occur as a result of uneven laser resurfacing or dermabrasion. With all modalities of resurfacing, care must be taken to ensure an even and homogeneous treatment.

Fig. 6.1 Excess skin wounding from overcoating with Jessner’s solution.
Dyspigmentation can occur after any depth chemical peel, but deeper peel procedures harbor risk of greater problems. In general, patients with light complexions (Fitzpatrick skin types I–II) have lower risks for this complication, while Fitzpatrick IV–VI skin must be approached with caution due to the elevated risk of hyper-pigmentation. Patients taking photosensitizing drugs or hormone replacement therapy (estrogen) are also at greater risk for pigmentary complications from resurfacing procedures (Table 6.2), and therefore it is unwise to proceed until these medications have been stopped completely and the risk profile has decreased sufficiently (12 months after Accutane, for example).
Table 6.2 Common Photosensitizing Medications
Antibiotics • fluoroquinolones (ciprofloxacin, levofloxacin, gatifloxacin) • tetracyclines (tetracycline, doxycycline, minocycline) • sulfonamides (sulfamethoxazole, trimethoprim, cotrimoxazole) Antihistamines • diphenhydramine Antimalarials • quinine • chloroquine • hydroxychloroquine Chemotherapeutic agents • 5-fluorouracil • vinblastine • dacarbazine Cardiac agents • amiodarone • nifedipine • quinidine • diltiazem Diuretics • furosemide • hydrochlorothiazide Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|