73
Rheumatoid Arthritis: Metacarpophalangeal Joint Reconstruction Arthroplasty
R. John Naranja, Jr. and Kevin D. Plancher
History and Clinical Presentation
A 53-year-old right hand dominant woman was originally diagnosed with rheumatoid arthritis 14 years ago. Medical management of her disease process has included chronic oral prednisone. Her primary complaint includes pain and deformity of her hands and decreased function secondary to lack of mobility and strength.
Physical Examination
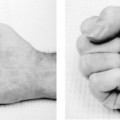
The patient has ∼25 degrees of ulnar drift at the index through small finger metacarpophalangeal (MP) joints. An extension deficit at the MP measures ∼50 degrees (Fig. 73–1). The arc of motion of the digits at the MP joint is 20 degrees. Key pinch strength is 30 N and grip strength is 70 N at position II using the Jamar dynamometer. There is relative preservation of joint motion at the proximal interphalangeal (PIP) joint and wrist articulations without significant collapse or deformity.
PEARLS
- Meticulous detail is necessary when reaming the proximal phalanx of the little finger when there is poor bone stock and especially in patients with juvenile rheumatoid arthritis.
- When silicone synovitis and loss of bone stock occur, a resection arthroplasty should be considered.
PITFALLS
- Inadequate soft tissue balancing and poor hand therapy can lead to recurrence of the deformities and subluxation of these joints.
- Use of silicone implants can lead to an inflammatory response with subsequent erosive changes.
Diagnostic Studies
Radiographs of the hand to include posteroanterior (PA) (Fig. 73–2), lateral, and oblique views demonstrate subluxation and joint destruction of the MP joints in the index through small fingers of the right hand. Though there is relative diffuse osteopenia present, adequate bone stock appears present for potential implant arthroplasty.

Figure 73–1 A classic ulnar drift and extension deficit in a rheumatoid hand seen at the metacarpophalangeal joints. (Illustration courtesy of The Indiana Hand Center and Gary Schnitz.)

Figure 73–2 Posteroanterior (PA) radiograph of metacarpophalangeal (MP) subluxation and joint destruction.
Differential Diagnosis
Degenerative joint disease
Rheumatoid arthritis
Septic joints
Diagnosis
Rheumatoid Destruction and Deformity of the Index through Small Finger Metacarpalphalangeal Joints
The MP joint in the rheumatoid hand is commonly affected by joint destruction and deformity. Typically, the disease process involves bony articular destruction, and ulnar and volar capsular contracture with concordant radial capsular attenuation. This subsequently results in subluxation of the flexor sheath in an ulnar and volar direction in addition to ulnar displacement of the common extensor tendon. Intrinsic tightness contributes to overall dysfunction. Indications for arthroplasty reflect the disease process and include pain and disability with radiographic evidence of joint destruction, limited MP range of motion secondary to contracted myotendinous and ligamentous supports, ulnar drift that has failed other soft tissue procedures, and stiff distal interphalangeal (DIP) or PIP joints. Arthroplasty of the MP joint predictably addresses these processes and maintains function better than arthrodesis or simple resectional arthroplasty in patients with adequate bone stock, soft tissue coverage, and absence of preexisting infection.
Surgical Management
A transverse or longitudinal skin incision is created dorsally over the region of the metacarpal necks. The dorsal veins are preserved and the extensor hoods to each digit are exposed with care to protect the neurovascular structures radially and ulnarly. The extensor tendon is identified and is usually subluxed ulnarly with attenuation of the extensor tendon at its radial aspect (Fig. 73–3
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


