Key Words
replantation, revascularization, amputation, fingertip or digit amputation
Synopsis
The term replantation is used when there is surgical reattachment of a completely amputated body part. In contrast, when there is some tissue still attached, and reattachment of this incompletely amputated part requires microsurgical repair of the vessels, this is called revascularization.
Malt and McKhann performed the first successful upper arm replantation in 1962, and Komatsu and Tamai reported the first successful replantation of a digit in 1968. Since then, microsurgery and replantation have been a basic part of training and routine practice for hand surgeons. Even the best available hand prosthesis has not been able to entirely replicate the function of the hand as effectively as prostheses for the lower extremities. Furthermore, cultural and religious practices in certain countries place a particular emphasis on the presence of all body parts upon death. Therefore replantation is becoming increasingly important in all countries, regardless of socioeconomic conditions.
Although microsurgery has seen considerable advances in recent years, hand surgeons have been increasingly critical with regard to outcomes of replantation. It is vital to understand that the successful outcome of the replantation does not just depend on microsurgical repair of the vessels but also on restoration of bone, tendon, nerve, and skin. Tendon repair is likely to be the most important step for better long-term outcome of the replantation.
Clinical Problem
The need for a detailed history focuses on the health of the patient and the cause of the amputation. The key points to be considered are enumerated later, and a summary of the relative indications and contraindications is listed in Table 5.8.1 .
| Indications | Contraindications |
|---|---|
|
|
Age
Younger patients may have better outcomes with nerve and tendon repair. Children may have more technically demanding surgery because of the small caliber of the vessels. Older patients are more likely to have systemic diseases and atherosclerosis of the vessels.
Occupation
The patient’s occupation and hobbies may help determine whether s/he requires gross or fine motor function of the hand. For example, a construction worker may be better served by a completion amputation and early return to work, whereas a pianist may wish all efforts at replantation to be made.
Associated Injuries
If the amputation is associated with life-threatening major injuries, it may be wise not to perform replantation. The overall patient is more important than the digit.
Warm Ischemia Time
This is more critical for major replantation in the hand and more proximally, where there is significant muscle that may become ischemic. Amputation proximal to the radio-carpal joint results in irreversible changes leading to myoglobinuria and renal failure if replanted beyond 6 hours of warm ischemia time. However, this time length is much longer in a finger, where there is very little muscle tissue.
Etiology and Mechanism of Injuries
A detailed history of the mechanism of injury provides information to foreseeing the severity of injury and the likelihood of success. Sharp cut or guillotine amputations have clean margins and are best suitable for replantation, whereas crush and avulsion injuries may have tissue loss and multiple-level injuries. Wound contamination increases the risk of infection and requires radical debridement.
Associated Conditions
Associated comorbidities such as diabetes, coronary artery disease, chronic obstructive pulmonary disease, history of smoking, drug dependence, and psychiatric illness are negative factors for replantation.
Pre-Operative Management
Physical Examination
Examining the patient as a whole is very important. There is a tendency to mistakenly exclude other pertinent signs that may lie outside our area of expertise. However, general examination should always precede the focused examination because it helps avoid the risk of missing the major injuries. In cases of trauma, a full body survey should be performed to rule out other injuries.
General Examination
Determining the general health of the patient is critical for pre-operative decisions such as the specific procedure, required preparation, and type of anesthesia. In most cases of replantation, the patient should be healthy enough for a long time period of general anesthesia.
Regional Examination
The whole limb should be examined so as not to miss proximal injuries.
Focused Examination
Both the limb and the amputated part should be examined thoroughly. It is typically better to conduct the gross examination during the initial presentation of the patient in the emergency department, followed by a thorough, detailed evaluation in the operating room. This approach saves time and reduces the unnecessary hassles of insufficient lighting and supplies.
Factors Requiring Evaluation
- •
Single-digit vs multiple-digit injury
- •
Level of amputation
- •
Clean cut vs crush/avulsion mechanism
- •
Amount of contamination
Counseling
Patients and their relatives almost always desire the replantation of any part of their body. However, they are typically not aware of the required procedure in detail, its associated risks, the cost, and the potential complications and outcomes of the surgery. It is therefore the responsibility of the operating surgeon to discuss the proposed procedure in detail so as to facilitate the making of well-informed decisions by the patient. The likelihood of completion amputation should be emphasized.
Topics to Be Discussed
- 1.
Duration of surgery, post-operative therapy, and length of hospital stay.
- 2.
Likelihood of success.
- 3.
Possibility of multiple surgeries for re-exploration, re-revascularization, and secondary surgeries.
- 4.
Possible need for blood transfusion.
- 5.
Possible need for skin, vessel, and nerve grafts.
- 6.
Intensive rehabilitation and time off from work,
- 7.
Expected outcome in terms of function, appearance, and sensibility.
- 8.
Cost.
- 9.
Options of alternate surgeries and their outcomes, including completion amputation.
Investigations
Routine tests should be performed to determine the general health of the patient, risks and complications of blood loss, and suitability for the procedure. Tests, depending on individual need, include:
- 1.
Basic blood tests:
- a.
Complete blood count
- b.
Blood type and crossmatch for major replantations
- c.
Renal function test if indicated
- a.
- 2.
Radiograph
- a.
x-ray of the proximal extremity and the amputated part should be taken
- b.
Chest x-ray if indicated
- a.
- 3.
Electrocardiogram if indicated
Emergency Management and Preparation
The patient should be stabilized before being taken to surgery.
- 1.
Analgesia
Adequate analgesia should be given because excessive pain results in vasoconstriction. It also has the added benefit of reducing patient anxiety.
- 2.
Tetanus prophylaxis
This should be given if the booster dose has been given at least 5 years prior or if the immunization history is uncertain.
- 3.
Antibiotics
A first-generation cephalosporin usually suffices. Aminoglycoside and metronidazole can be administered if indicated, in cases of severe contamination. Penicillins should be administered in the case of farmyard injuries.
- 4.
Blood and fluids
Patients with amputations, especially above the radio-carpal joint, are at a high risk of losing significant amounts of blood at the amputation site. Blood transfusions may therefore be necessary. Patients should be well hydrated to reduce the likelihood of hyperviscosity.
- 5.
Urinary catheter placement
Replantation procedures are typically long in duration, and an indwelling catheter is therefore recommended. This has the added benefit of serving as a useful indicator of the patient’s hydration status intraoperatively and post-operatively.
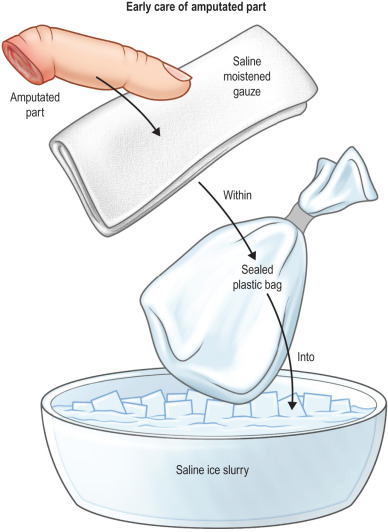
- 6.
Preparation of the amputated part
The parts should be irrigated and wrapped with saline-soaked gauze. The part is then placed in a plastic bag, which is then placed in an ice bath. This allows cooling of the part while avoiding direct contact with ice or saline ( Fig. 5.8.1 ).