Rejuvenating the hands can have a significantly beneficial impact on a patient’s overall esthetic journey. One of the key hallmarks of natural-looking results from cosmetic procedures is ensuring continuity with areas of the body that easily reveal one’s age. This article will review the multifaceted components of the aging hands as well as provide a detailed guide on treatments and best practices to improve photodamage, volume loss, skin quality, and unwanted veins and on how to combine procedures to optimize treatment results.
Key points
- •
The dorsal hands are an overlooked anatomic area for cosmetic procedures.
- •
One hallmark of natural-looking results from cosmetic procedures is ensuring continuity with areas of the body that easily reveal one’s age.
- •
Understanding the anatomy of the hand is paramount to formulate a treatment plan and deliver safe and effective results.
- •
Optimizing overall skin quality with treatments focused on improving of photodamage, volume loss, and unwanted veins should be the focus of every consultation.
Introduction
The dorsal hands are often an overlooked anatomic area for cosmetic procedures despite much effort to beautify this area by embellishing the nails with polish or adorning the fingers and wrists with jewelry. Rejuvenating the hands can have a significantly beneficial impact on a patient’s overall esthetic journey and should be considered in a comprehensive consultation. All too often, the majority of the focus of cosmetic procedures is on the face resulting in a stark discontinuity between the refreshed face and an aged appearance of other cosmetic units such as the dorsal hands. One of the key hallmarks of natural-looking results from cosmetic procedures is ensuring continuity with areas of the body that easily reveal one’s age. This article will review the multifaceted components of the aging hands as well as provide a detailed guide on treatments and best practices to improve photodamage, volume loss, skin quality, unwanted veins, and how to combine procedures to optimize treatment results.
The aging hands–assessment and consultation
The thin, delicate skin of the dorsal hands is extremely vulnerable to the aging process due to their constant exposure to extrinsic environmental elements, most notably ultraviolet radiation from the sun, but also from the constant barrage of other insults from day-to-day wear and tear such as exposure to water, chemicals, and smoking, among many others [ ]. Intrinsic factors from chronologic age and one’s genetics also play a role in how the hands will age [ ].
Youthful hands are characterized by thick, durable skin that is volumized and without atrophy and wrinkles [ ]. Additionally, veins, tendons, and bony outlines are minimally visible. The skin is evenly toned without blemishes.
Aged hands exhibit atrophy and loss of volume of the subcutaneous tissue revealing prominent veins, tendons, and bones [ ]. The overlying skin is typically wrinkled and heterogeneous in color and texture displaying mottled dyspigmentation, solar lentigines, seborrheic keratoses, actinic keratoses, and/or skin cancers [ , , ]. The skin may also be vulnerable to injury and bruising.
Anatomic considerations
The dorsal hand is a delicate anatomic structure; the dermal thickness ranges from just 0.2 mm to 0.9 mm [ , ]. The dorsal hand is made up of 3 separate fatty laminae—superficial, intermediate, and deep—each separated by a fascial layer [ , ]. The veins and nerves reside in the intermediate lamina and the extensor tendons are located in the deep lamina [ ]. The superficial dorsal lamina located between the dermis and dorsal superficial fascia, unlike its intermediate and deep counterparts, does not contain any blood vessels or nerves making it the ideal location for injection of dermal fillers, biostimulators, and fat [ , , ]. This superficial dorsal lamina, however, was found to have septal adhesions which contain perforating vessels, which if dissected can cause bleeding and subsequent bruising [ ]. The main purpose of this superficial compartment is to provide protection and support to the underlying layers which contain vessels, nerves, and tendons [ ]. To ensure one is in this safe zone when performing volumizing procedures, it is helpful to “scrape the dermis,” a technique demonstrated by Lefebvre-Vilardebo et al to ensure placement of product in the correct superficial plane [ , ]. Use of cannulas can be extraordinarily helpful in localizing the proper tissue plane as the cannula will start to glide immediately below the dermis. The optimal landmarks for injection of fillers and biostimulators lie between the dorsal crease of the wrist proximally to the metacarpophalangeal joints distally and bound laterally by the fifth metacarpal and medially by the second metacarpal [ , ].
Skin
General Considerations
There are many modalities that can improve sun damage as well as skin tone and texture. It is imperative to keep in mind the following when choosing an appropriate treatment modality.
- 1.
Fitzpatrick skin type of the patient—Not all laser and light-based devices are safe for every patient. Ensure the appropriate laser or device is utilized for the patient’s skin complexion.
- 2.
Thoroughly examine the lesions to be treated. Suspicious pigmented lesions should not be treated with any laser or light-based device. Dermoscopy can be helpful in examination of concerning lesions, if the practitioner has the requisite expertise. Lesions concerning for a skin cancer should be appropriately investigated or referred to a board-certified dermatologist.
- 3.
Settings—Ensure the appropriate device settings are utilized, keeping in mind the patient’s skin type and remembering treatment is off-face. The skin of the hands is not as forgiving as that of the face due to its thin quality and lack of robust adnexal support structures [ ]. Device settings should typically be reduced from those used on the face. Moreover, multiple treatment sessions may be necessary since more conservative settings are typically needed.
- 4.
Healing time—The skin of the hands lacks many adnexal structures, healing will take longer.
- 5.
Aftercare—As with any treatment, post-procedure care is imperative to ensure a safe and optimal result. Bland emollients and sunscreen should be used at a minimum.
- 6.
Fully ablative lasers will not be discussed; these devices are not an optimal treatment modality as the relative lack of adnexal structures reduces the ability to heal. These devices have a low threshold for scarring if not used with meticulous expertise.
Q-switched and Picosecond Lasers
Seven hundred and fifty five nm Alexandrite, 694 ruby, and frequency-doubled 532 nm Nd:YAG lasers can all be used to treat discrete solar lentigines and/or macular seborrheic keratoses [ ]. Using the principle of selective photothermolysis, the light emitted by these lasers with wavelengths between 500 and 755 nm is selectively absorbed by the chromophore, melanin, without damage to surrounding skin structures [ , , ]. Very short pulse durations are needed to correspond to the short thermal relaxation time of melanosomes which is in the range of 10 ns to 1 μs, making Q-switched (QS) and picosecond lasers ideal modalities [ , , ].
With the advent of picosecond lasers in 2012, these lasers can be utilized to treat photodamage in a variety of skin types. Picosecond lasers break up the target chromophore utilizing both photomechanical and photothermal effects [ ]. These lasers have a more favorable safety profile especially when treating higher Fitzpatrick skin types [ ]. Picosecond lasers with a diffractive lens array create a photoacoustic wave and subsequent laser-induced optimal breakdown allowing for improvement of not only dyspigmentation but also collagen stimulation [ ].
Technique
- •
The appropriate endpoint is uniform whitening of the treated lesion with no change to the surrounding skin and without epidermolysis [ ].
- •
A smaller spot size requires higher energy fluence. A small spot size with high energy should be reserved for lighter Fitzpatrick skin types to diminish adverse effects.
- •
Lower fluences should be utilized when treating patients of high Fitzpatrick types [ ].
- •
The lighter the color of the targeted lesion the higher the fluence will be necessary to achieve the endpoint.
- •
When using a picosecond laser for treatment of solar lentigines, 532 nm or 755 nm wavelengths can be utilized in Fitzpatrick I–IV with a preference for 532 nm for lighter lentigines and 755 nm for darker lentigines [ ]. The endpoint should be a light white frost [ ]. Treating Fitzpatrick V–VI skin types is challenging with a narrow window to achieve the appropriate endpoint while also avoiding pigmentary alteration of background skin; however, one can cautiously use a 730 nm, 755 nm, or 785 nm laser with low fluence [ ].
Clinical pearls and potential adverse events
- •
QS lasers work exceedingly well with minimal adverse effects in Fitzpatrick skin types I–III. Expert knowledge is required for treatment of Fitzpatrick skin type IV. Skin types V and VI should not be treated with QS lasers as there is a high risk of depigmentation.
- •
Adverse events include erythema, hyperpigmentation, hypopigmentation, scarring or textural irregularities, and bullae formation [ ]. Hyperpigmentation and hypopigmentation is a greater risk in higher Fitzpatrick skin types [ ].
Intense Pulsed Light
Intense pulsed light (IPL) emits a broad spectrum of wavelengths between 515 and 1200 nm, allowing this versatile device to treat both red and brown pigmentation [ , , , ]. There is even some evidence that there can be collagen stimulation by heating of the dermis during treatment [ , , , ]. These devices have a variety of cutoff filters which allow the practitioner to select different targets and depth of penetration [ ]. Cutoff filters remove all wavelengths below a specified wavelength [ ]. Although IPL systems have a pulse duration in the millisecond range, longer than the thermal relaxation time of melanosomes, this device can be used successfully to improve solar lentigines over multiple treatment sessions [ ]. This no downtime treatment makes it ideal for many patients.
Technique
- •
Cooling the skin appropriately during this treatment is important. The authors like to use a thin layer of cooled ultrasound gel applied to the treatment zone. In addition to the cooled tip of the device, cold air cooling (Zimmer MedizinSystems; Irvine, CA) is utilized. These cooling techniques not only add to the patient’s comfort during treatment but also heighten safety of the treatment.
- •
Approximately 10% to 20% overlap is utilized to ensure an even treatment without skip areas.
- •
Appropriate selection of pulse duration, pulse delay, and fluence requires knowledge of the target, skin Fitzpatrick type, and anatomic area.
Clinical pearls and potential adverse events
- •
The authors usually forgo the use of topical numbing cream for IPL treatments. Topical numbing cream can superhydrate the skin which can diminish any potential collagen stimulation from the IPL device.
- •
The 560-nm filter is the workhorse wavelength utilized by the authors. This filter can target both brown pigment as well as background erythema.
- •
If brown pigment is targeted exclusively, then a 515-nm filter can be useful.
- •
A filter between 515 nm to 590 nm will effectively target vasculature [ ].
- •
When choosing the appropriate pulse duration, the authors like to use 3 millisecond when targeting melanin, 3.5 millisecond when targeting both melanin and vessels, and 4 millisecond when targeting vessels exclusively.
- •
Pulse delay should be adjusted based on the patient’s skin type and anatomic area. For patients with darker skin, increase the pulse delay. Additionally, when treating anatomic areas such as the hands where the skin is thin and lacks robust adnexal structures, a longer pulse delay is typically chosen.
- •
When treating the hands, the fluence is typically dropped by 1–2 J/cm 2 as compared to energies used for the face [ ]. Other indications to reduce fluence further are Fitzpatrick skin type, recent tanning, and a patient’s pain during treatment. Signs of over treatment include excessive redness, swelling, and/or burning which may be delayed and not appear right after the treatment has concluded.
Non-ablative Fractional Lasers
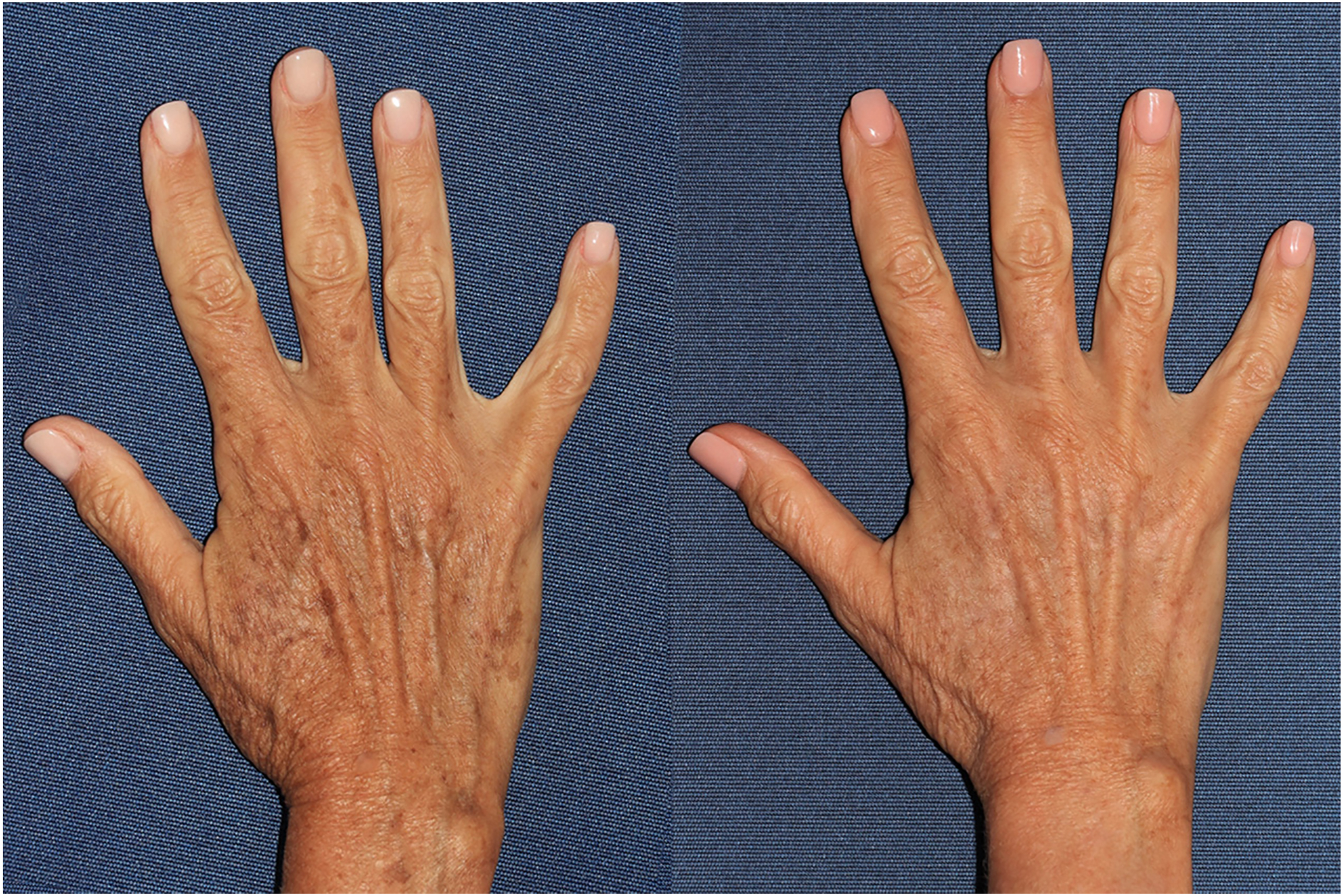
Non-ablative mid-infrared fractional lasers such as the 1550- nm erbium-doped and the 1927 nm thulium lasers (Fraxel Re:Store Dual; Solta Medical, Inc.; Bothell, WA) are commonly used for improvement of skin texture and photorejuvenation, respectively [ ]. All Fitzpatrick skin types can be treated with these lasers with the use of appropriate parameters. The 1550 nm wavelength is utilized to improve skin texture by stimulating collagen production [ ]. The 1927 nm is best utilized for improvement of photodamage ( Figs. 1 and 2 ) [ ].

Technique
- •
Topical numbing for 60 minutes is recommended. Prior to laser treatment, it is recommended to cleanse the treatment zone with isopropyl alcohol and/or Hibiclens (chlorhexidine gluconate solution 4%; Mölnlycke Health Care AB; Gothenburg, Sweden) [ ].
- •
When utilizing the 1927 nm wavelength, the authors prefer the following parameters: fluence between 10 to 20 mJ, 30% to 50% coverage (adjust according to skin type), and 8 passes [ , ].
- •
When utilizing the 1550 nm wavelength, the authors prefer the following parameters: 15 mm handpiece, fluence between 25 to 35 mJ, ≤23% coverage (Fitzpatrick skin types I-III) or 9% to 17% coverage (Fitzpatrick skin types IV-VI), and 8 passes [ , ].
- •
Multiple treatment sessions are recommended spaced 4 to 6 weeks apart.
Clinical pearls and potential adverse events
- •
The authors prefer not to use both the 1550 nm and 1927 nm wavelengths in the same treatment as settings for both will need to be reduced.
- •
If both wavelengths are used, it is recommended to treat skin texture with the 1550 nm followed by the 1927 nm wavelength. Additionally, if both wavelengths are utilized appropriate down titration of laser settings is imperative to deliver a safe treatment.
- •
Post-treatment, erythema and swelling is anticipated.
- •
Prevention of bulk heating is imperative; repeated back and forth motions within small areas should be avoided [ ]. Ensure appropriate cooling of skin for added safety.
Ablative Fractional Lasers
Although there are numerous non-ablative modalities that can rejuvenate the hands with considerably less downtime, the use of fractional ablative carbon dioxide or erbium lasers can be utilized to improve dyschromia as well as texture. These lasers vaporize columns of skin to specific depths. By treating only a fraction of the total surface area, the healing time is shorter and the treatment is safer than traditional fully ablative devices. Areas of untreated skin act as reservoirs for fibroblasts and adnexal structures to heal areas of ablation [ ].
Clinical pearls and potential adverse events
- •
This treatment is not advised for higher Fitzpatrick skin types.
- •
Choosing the appropriate fluence will dictate depth of ablation. Remembering that the skin of the dorsal hands is thinner than other areas such as the face is paramount.
- •
Lower densities and fluence should be utilized as the skin in this anatomic area is not as resilient as the face. The risk of scarring with high settings is a possibility.
- •
Healing time can be longer with more post-laser erythema than if non-ablative modalities are utilized.
- •
Because of the low settings required to reduce adverse events and prolonged healing, the risk/benefit ratio may not favor treatment with ablative lasers.
Photodynamic Therapy
Photodynamic therapy (PDT) involves the application of a photosensitizer such as 20% aminolevulinic acid (ALA) which is then activated by a variety of laser and light devices such as pulsed dye laser, IPL, as well as red and blue light [ , , ]. Any laser or light source within the visible light spectrum can activate the photosensitizer [ ]. Activated ALA will generate reactive oxygen species that will subsequently cause apoptosis of targeted skin cells [ ]. Although PDT is typically utilized for the treatment of actinic keratoses (AKs) and superficial keratinocyte carcinomas, this treatment modality can be very effective in photorejuvenation by improving mottled pigmentation and even improving skin texture [ , , ].
Technique
- •
ALA is applied to the dorsal hands following degreasing with isopropyl alcohol and exfoliation with a vibrating microdermabrasion system (Vibraderm; Grand Prairie, TX) [ , ].
- •
The ALA is typically incubated for 60 minutes [ , ]. Following the incubation, the hands are washed with a gentle cleanser to remove the ALA [ ].
- •
To activate the ALA, a pulsed dye laser (PDL) is first utilized for treatment of visible AKs. The authors’ typical settings for a 585 nm PDL (Cynergy, Cynosure; Westford, MA) are 7 mm spot size, 40 millisecond pulse duration, and 10–12 J/cm 2 [ , ].
- •
IPL is then utilized, the authors’ typical settings for Fitzpatrick skin types I–III (M22, Lumenis Ltd.; Yokneam, Isreal) are 560 nm filter, double pulse durations of 3.5 millisecond with a 20–30 millisecond pulse delay, and a fluence range of 16–18 J/cm 2 [ , ].
- •
Finally, the treatment zone is illuminated with blue light (417 nm) for 16 minutes and 40 seconds at 10 J/cm 2 as well as red light (635 nm) for approximately 8 minutes [ , ].
Clinical pearls and potential adverse events
- •
Patients should refrain from sun exposure for approximately 48 hours post-treatment [ ].
- •
Two to three PDT sessions, spaced 1-month apart, are often required for treatment of AKs [ ].
- •
Consideration can be given to priming hands with actinic damage with 5 days of 5-fluorouracil (5-FU) or other topical agents prior to PDT.
Volume
Revolumizing the dorsal hands can make this highly visible area more youthful by improving volume-depleted, crepe-like, and wrinkled skin as well as camouflaging prominent veins, tendons, and bones [ ].
Hyaluronic Acid Fillers
A 20 mg/mL, 750–1000 μm particle-sized non-animal-derived stabilized hyaluronic acid (NASHA) hyaluronic acid filler with minimal cross-linking (Restylane Lyft; Galderma Laboratories; Fort Worth, TX) is the only hyaluronic acid (HA) filler FDA-approved for dorsal hand rejuvenation [ , ]. Results from treatment with this 20 mg/mL HA filler were maintained up to 12 months using an average of 2.1 mL per hand [ ]. Although off-label, other HA fillers that can be used for augmentation of the hands include a 17.5 mg/mL Vycross product (Juvéderm Vollure; Allergan Aesthetics; Irvine, CA) as well as a 24 mg/mL Hylacross product (Juvéderm Ultra Plus; Allergan Aesthetics; Irvine, CA) [ ].
Biostimulators
Calcium hydroxylapatite (CaHA)(CaHA, Radiesse; Merz North America, Inc.; Raleigh, NC) and poly- l -lactic acid (PLLA, Sculptra Aesthetic; Galderma Laboratories; Fort Worth, TX) are considered biostimulators because they will develop one’s own collagen (types I and III) by stimulating the body’s fibroblasts [ ].
CaHA was FDA-approved for correction of volume loss of the dorsal hands in 2015 and remains the only biostimulator approved for this indication [ ]. CaHA microspheres, which measure approximately 25–45 μm, are suspended in a carboxymethlycellulose gel carrier and are biocompatible [ , , , ]. Not only will CaHA provide instant volumization for the hands but will also stimulate collagen production over approximately 4 to 6 months which will further improve skin quality, particularly the crepe-like changes seen as one ages. CaHA typically lasts 1 year; however, this is variable and in the pivotal trial, 68% of the patients maintained their result at 1-year post-injection [ , , ]. Additionally, since CaHA is an opaque white color, it will also diminish the appearance of the tendons and blue veins [ , ].
Although PLLA can be used to rejuvenate the dorsal hands, albeit off-label, it is not the biostimulator of choice of the authors. The dorsal hands with its intricate network of constantly moving tendons makes the risk of nodule formation of the PLLA particles a potential threat to an optimal outcome [ , ]. Nodule formation has been demonstrated even after just 1 treatment [ ]. Additionally, unlike CaHA or a traditional HA filler, the results of PLLA are not instant nor accomplished in 1 treatment session as it works exclusively to stimulate the body’s own collagen to improve volume and skin quality. If used, PLLA typically requires approximately 3 to 4 treatment sessions spaced 4 to 6 weeks apart; results can last between 18 to 24 months [ , ]. An adequate reconstitution of PLLA with at least 16 cc of diluent is recommended to diminish the risk of nodule formation, an increase from the previously recommended 5–8 cc dilution [ , , ].
Technique
- •
Use of a blunt-tipped cannula (25G or 22G 2″ are preferable) can help diminish bruising and increase safety with injecting [ ]. For added comfort, use of injectable lidocaine with epinephrine for pilot needle entry is helpful. Tent up the skin to ensure exact placement of the pilot needle into the superficial laminary compartment where the superficial fat is located [ ].
- •
Ensure that the extrusion hole of the cannula is oriented upwards toward the dermis to further ensure the product is injected subdermally [ ].
- •
Retrograding fanning technique will allow placement of product easily and evenly, parallel to the extensor tendons [ , ].
Clinical pearls and potential adverse events
- •
Needles can be used to deliver the product; however, the potential for bruising is much higher and one needs to ensure that vessels in the treatment zone are not injected. A depot injection will require adequate massage to ensure even dispersal of the product [ ]. If using a needle, first tent up the skin to ensure injection of the filler product is superficial and the skin is separated from underlying vascular and tendinous structures [ , ].
- •
In a retrospective study, it was demonstrated that adverse events occurred in 23.9% of the cases treated with needle compared with 3.1% treated with cannula [ ]. In the same study, the proximal-to-distal fanning technique had the least adverse events compared to the distal-to-proximal technique or the bolus technique when placing an injectable product [ ].
- •
The authors prefer to place the pilot needle entry point inferior to the wrist and direct the cannula toward the metacarpophalangeal joints.
- •
After 1 hand is injected, the authors like to wrap the treated hand in a disposable pad and have the patient sit on their hand while the other hand is being injected [ ]. This can help to smooth out the injectable and reduce bruising.
- •
Revolumizing the fingers may be requested by some patients; however, this technique is high risk. The fingers are a closed compartment which when injected can potentially cause joint mobility issues and/or compartment syndrome. The medial and lateral aspects of the fingers should be avoided as the dorsal digital vasculature course in this area [ ].
- •
Care must be maintained when injecting in and around the knuckles as there have been reports of vascular occlusion due to injection of the proper palmar digital arteries [ ].
- •
Do not overfill the hands as this will give an unpleasant “doughy” appearance.
- •
The authors like to blend one 1.5-mL syringe of CaHA with approximately 0.5 to 1.5 cc of either normal saline or lidocaine without epinephrine ( Figs. 3 and 4 ) [ ]. Blending the CaHA will allow the injectable to be more malleable and less viscous [ , ]. The authors also like to blend approximately 0.5 cc of normal saline with either Juvéderm Vollure or Ultra Plus.