The overhead throwing athlete possesses distinct physical traits and undergoes adaptive changes due to the repetitive nature of throwing, often resulting in significant injury to the shoulder or elbow joint. An effective rehabilitation program for the throwing athlete is dependent upon an accurate evaluation that identifies the causative factors contributing to the athlete’s condition. In this article, we outline the unique physiology of the thrower’s shoulder and elbow, the injuries associated with these athletes and a multiphased rehabilitation approach that allows for the restoration of strength, mobility, endurance, and power essential to return to unrestricted overhead sporting activity.
Key points
- •
The overhead thrower displays unique range of motion (ROM), postural, strength, and joint mobility characteristics that occur as a result of physical adaptation to the imposed stresses and demands of repetitive throwing.
- •
The success of the rehabilitation program is dependent upon an accurate recognition of the underlying cause of the pathology. The program is individualized based on the athlete’s diagnosis, evaluation, and goals.
- •
An effective rehabilitation program will focus on re-establishing full full throwing ROM, dynamic rotator cuff stability, scapulothoracic control, and muscular endurance, while implementing a progressive resistance exercise program that progressively challenges the athlete preparing them to return to throwing.
The shoulder and elbow joints are common sites of pathology in the baseball player. The frequency of repetitive stress injuries in the overhead athlete, particularly baseball pitchers, continues to increase. Major League Baseball (MLB) pitchers are the most injured players. Conte and colleagues reported that shoulder injuries represented 27.8% of all disabled list (DL) days in professional baseball players while elbow injuries account for 22% to 26% of all pitchers’ injuries. Based upon DL days, Posner and colleagues noted that pitchers in MLB experienced a 34% higher injury rate compared to fielders, and when a pitcher was placed upon the DL for injuries to the upper extremity, their absence lasted for a longer duration (74.25 days vs 54.15 days). Recently, Conte (presentation at 2024 Injuries in Baseball Course) reported that in 2023 MLB spent US$1.1 billion on players on the injured list (IL).
According to the National Collegiate Athletics Association (NCAA) Injury Surveillance System from 1998 to 2004, for all injuries that lasted 10 or more days, shoulder strains/tendinitis equated to 8.2% of all injuries occurring during games and 16.7% of injuries during practice. The shoulder has also been reported to be the most injured region in high school baseball players, representing 34.2% of all injuries in pitchers and 24.9% in catchers with an overall prevalence of 17.6% for all positions.
Shoulder and elbow injuries are common due to the repetitive nature of overhead throwing. Tremendous forces are placed across the shoulder and elbow joints as angular velocities reach 7250°/s during throwing. Anterior shear forces at the shoulder approach 50% body weight during the throwing motion. Elbow extension occurs at more than 2300°/s, producing a medial sheer force of 300 N and a compressive force of 900 N creating a valgus elbow stress 64 N m during the acceleration phase of throwing, which exceeds the ultimate tensile strength of the ulnar collateral ligament (UCL), potentially causing osteophytes posteriorly, olecranon stress fractures, and physeal injuries. , ,
High levels of muscular activity are also generated during the throwing motion with forces reaching 120% maximal volitional isometric contraction. Although an inherent degree of mobility is needed to achieve the extreme arc of motion necessary to throw, the thrower depends on dynamic stability to minimize the potential for injury. Therefore, an essential balance between mobility and stability is needed to maintain joint integrity during high levels of extreme torque.
The rehabilitation program for the throwing athlete described in this article follows a multiphased, systematic approach focused on a return to prior level of function. This program is divided into 4 phases designed to allow a gradual progression of exercises and imparted stresses that methodically build on the previous exercises designed to restore strength, increase dynamic stability, and develop neuromuscular control. Critical to the successful restoration of function in the thrower is the identification of the causative pathologic factors unique to each player and implementing an individualized treatment program designed to address them.
This article will describe a rehabilitation program for the throwing athlete that can be applied to both conservative and operative conditions of the shoulder or elbow. Additionally, we will outline the postoperative rehabilitation milestones for common shoulder and elbow procedures in the throwing athlete.
Rehabilitation program framework
This framework aims to provide a structure to address the causative factors common in the overhead thrower. Its success relies on a thorough clinical examination and appropriate sequencing through all phases of the rehabilitation process.
Phase 1: Acute Phase
The goals in this initial phase of the rehabilitation program are to diminish pain and inflammation, normalize range of motion (ROM), correct postural adaptations, normalize muscle balance, and re-establish baseline dynamic joint stability. During the acute phase of treatment, the athlete may be prescribed nonsteroidal anti-inflammatory drugs (NSAIDs) and/or undergo a local injection. Additionally, therapeutic modalities such as ice, iontophoresis, laser therapy, piezo wave therapy, and/or electrical stimulation may be used clinically to assist in the alleviation of pain and inflammation. The athlete is educated on activity modification/avoidance (including throwing, strenuous activities, and exercise performance) as well as sitting and standing postural education to increase subacromial space, appropriately activate postural musculature, and optimally position the athlete at rest.
Following the abating of acute inflammation, the rehabilitation specialist may implement the use of moist heat, ROM, and joint mobilization techniques aimed to increase local circulation of the joint capsule and surrounding soft tissues. Decreased electromyography (EMG) activity of 23% with a corresponding reduction of 32% external rotation (ER) force production has been documented in a painful shoulder. This lends credence to the importance of pain reduction to allow for the restoration of normal rotator cuff and upper quarter muscular recruitment.
The clinician may utilize soft tissue mobilization techniques with the goal of improving tissue extensibility, reducing pain and guarding, and preparing the athlete for physical activities. Active-assisted range of motion (AAROM), light manual stretches, and grade 1 and 2 joint mobilizations are performed to diminish pain and muscle guarding via stimulation of the type 1 and 2 mechanoreceptors.
During the acute phase of rehabilitation, the clinician should ensure the normalization of motion by incorporating AAROM, passive ROM, manual stretches, and joint mobilization techniques of both the shoulder and the elbow. Although all aspects of mobility should be assessed, it is common for the overhead throwing athlete to display a loss of internal rotation (IR) and horizontal adduction. The loss of IR is commonly described as glenohumeral internal rotation deficit (GIRD). The loss of IR of greater than 20° on the throwing shoulder compared to the nonthrowing shoulder has been implicated in shoulder and elbow injuries. Glenohumeral IR loss has been attributed to osseous adaptations, posterior rotator cuff tightness, posterior capsule tightness, and an anteriorly tilted scapula. , Additionally, a loss of full shoulder elevation has been linked to increased elbow stress. A proper clinical assessment to differentiate among these factors is essential for the clinician to implement the appropriate treatment interventions.
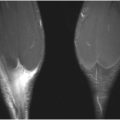
It is common for throwing athletes in, particular, to exhibit a loss of elbow extension after injury or surgery. , The elbow is predisposed to flexion contractures because of the intimate congruency of the joint articulations, the tightness of the joint capsule, and the tendency of the anterior capsule and brachialis to develop adhesions and scar following injury. ROM activities should be performed for all planes of elbow and wrist motions to prevent the formation of scar tissue and adhesions by providing nourishment to the articular cartilage and assisting in the synthesis, alignment, and organization of collagen tissue. , , Restoring full elbow extension is the primary goal of early ROM activities. At times, it can be difficult to regain full elbow extension and low-load, long duration (LLLD) stretch is needed to produce deformation or creep of the collagen tissue. This stretch can be performed by having the athlete lie supine with a towel roll placed under the distal humerus to act as a cushion and fulcrum. Light resistance exercise tubing is applied to the athlete’s wrist and secured to the table or to a dumbbell on the ground ( Fig. 1 ) as the athlete is instructed to relax for the duration of 10 to 15 minutes of LLLD treatment. The amount of resistance applied should be of low magnitude to enable the athlete to perform the stretch for the entire duration of the treatment without pain or muscle spasm. Athletes are instructed to perform the LLLD stretches several times per day, equaling at least 60 minutes of total end range time to improve extension and reduce joint stiffness.

A postural assessment should be performed and scapular mobility assessed, as an anteriorly tilted scapula is frequently seen in overhead throwers. Postural assessment of the scapula often reveals a protracted, depressed, and anteriorly tilted position compared to the contralateral side. This positioning can create muscle weakness and/or inhibition of the scapular retractors resulting in an altered length tension relationship. In addition, pectoralis minor tightness, coracoid pain, and lower trapezius muscle weakness are often noted. The decreased flexibility of the pectoralis minor can cause symptoms including arm fatigue, pain, tenderness, and cyanosis due to neurovascular occlusion as these structures pass underneath this muscle. , The pectoralis minor muscle can be assessed for tightness by having the patient stand against a wall and measuring the distance from the wall to the anterior acromial tip. An asymmetry greater than 3 cm is considered abnormal. We commonly perform pectoralis minor muscle stretches with the scapula placed in a retracted and posteriorly tilted position with 30° of shoulder flexion as the humerus is placed in an abducted and ER position. ,
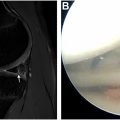
The posterior shoulder is subject to repetitive eccentric forces during throwing, which can result in increased internal stiffness and decreased ROM. The modified sleeper stretch ( Fig. 2 ), modified cross-body horizontal adduction stretch ( Fig. 3 ), and horizontal adduction stretch with concomitant IR are performed to improve flexibility of the posterior shoulder. The posterior capsule has been shown to exhibit significant laxity in throwers that exhibit GIRD; therefore, a proper evaluation should be performed to assess between capsular and soft tissue mobility. Mobilizations for the posterior capsule are performed parallel to the glenoid fossa in a posterior-lateral direction to increase pliability of the posterior capsule ( Fig. 4 ).


During this early phase of rehabilitation, strengthening exercises are initiated with the intention of restoring muscle balance/ratios and impeding muscle atrophy. , The aim of this phase is to re-establish dynamic stability; therefore, initial focus is on the innately weak rotator cuff and scapulothoracic musculature. , Eccentric control of the lower trapezius is essential in controlling scapular elevation and protraction as the arm decelerates, and weakness can result in improper mechanics leading to potential shoulder symptoms. The clinician may opt to initiate submaximal, pain-free isometrics during the acute phase in the presence of excessive pain and/or soreness, progressing to isotonics as tolerated. Rhythmic stabilization (RS) exercises are initially performed for the internal and external rotators with the arm in the neutral rotation and the shoulder in 30° of abduction. Manual cueing is used to facilitate cocontraction of the internal and external rotators to provide isometric stabilization of the glenohumeral joint during these exercises. These drills can also be progressed as the shoulder is placed in a “balanced position,” approximately 100° of elevation and 10° of horizontal abduction, which is beneficial because the rotator cuff and deltoid musculature resultant force vectors provide a centralized compression of the humeral head. , The athlete’s arm can be placed at various angles of both ER and elevation while applying manual cueing in various planes to facilitate recruitment of the surrounding musculature using this manual RS technique.
Proprioceptive sense can be diminished due to microtrauma or macrotrauma, thus the rehabilitation specialist should initiate techniques to heighten the sensory awareness of the afferent mechanoreceptors during this phase of rehabilitation. , Studies have demonstrated improvements in proprioception and enhanced functional throwing performance test scores following a 5 week program emphasizing neuromuscular and proprioceptive neuromuscular facilitation (PNF) training drills that challenge the glenohumeral musculature. , PNF movement patterns are performed while incorporating RS to the internal and external rotators to augment proprioception and dynamic stability. , , , , , Joint congruency is enhanced by facilitation of agonist and antagonist muscles, which assists in restoring a balance in the force couples of the shoulder joint complex. Joint repositioning drills and upper extremity axial loading exercises, such as weight shifts, weight shifts on a ball, wall push-ups, and quadruped drills are performed to stimulate the articular mechanoreceptors and aid in training proprioception during the early stages of treatment. , ,
Effective transfer of kinetic energy from the lower to the upper extremity is vital during throwing requiring adequate mobility, stability, and strength. Core and hip complex exercises are employed in this phase for postural re-education, stability, and mobility.
Phase 2: Intermediate Phase
The goals of phase 2 are to progress the strengthening program, while increasing the flexibility, mobility, and ROM of the entire upper quarter, while enhancing the athlete’s neuromuscular control. During this stage, the implementation of the Thrower’s Ten Program designed by Wilk and colleagues based-on EMG data facilitates the progression to more aggressive isotonic strengthening activities aimed at restoring muscle balance. Because the external rotators are commonly weak, side-lying shoulder ER and prone rowing into shoulder ER are prescribed due to the high EMG activity of the posterior cuff elicited during these movements.
Neuromuscular control drills are progressed as the clinician incorporates RS drills at the end ROM during the prior phase 1 movement drills. PNF exercises that are performed in a full arc of the patient’s available ROM serve to promote endurance training and dynamic stabilization of the rotator cuff. Manual resistance training can also be incorporated during this stage, allowing the clinician the ability to apply variable resistance throughout the movement, incorporate concentric and eccentric contractions, add RS during the exercise, and perform manual cueing for the scapular musculature.
The strength of the periscapular musculature is vital for optimal upper extremity function, as it provides proximal stability to allow for efficient distal arm mobility and has been described by several authors to contribute to normal overhead function.
Wilk and colleagues formulated specific exercises designed to normalize force couples of the scapular musculature and stimulate the proprioceptive and kinesthetic awareness to facilitate neuromuscular control of the scapulothoracic joint. The scapular retractors, protractors, and depressors are frequently emphasized due to commonly observed weakness of these muscle groups in the throwing athlete.
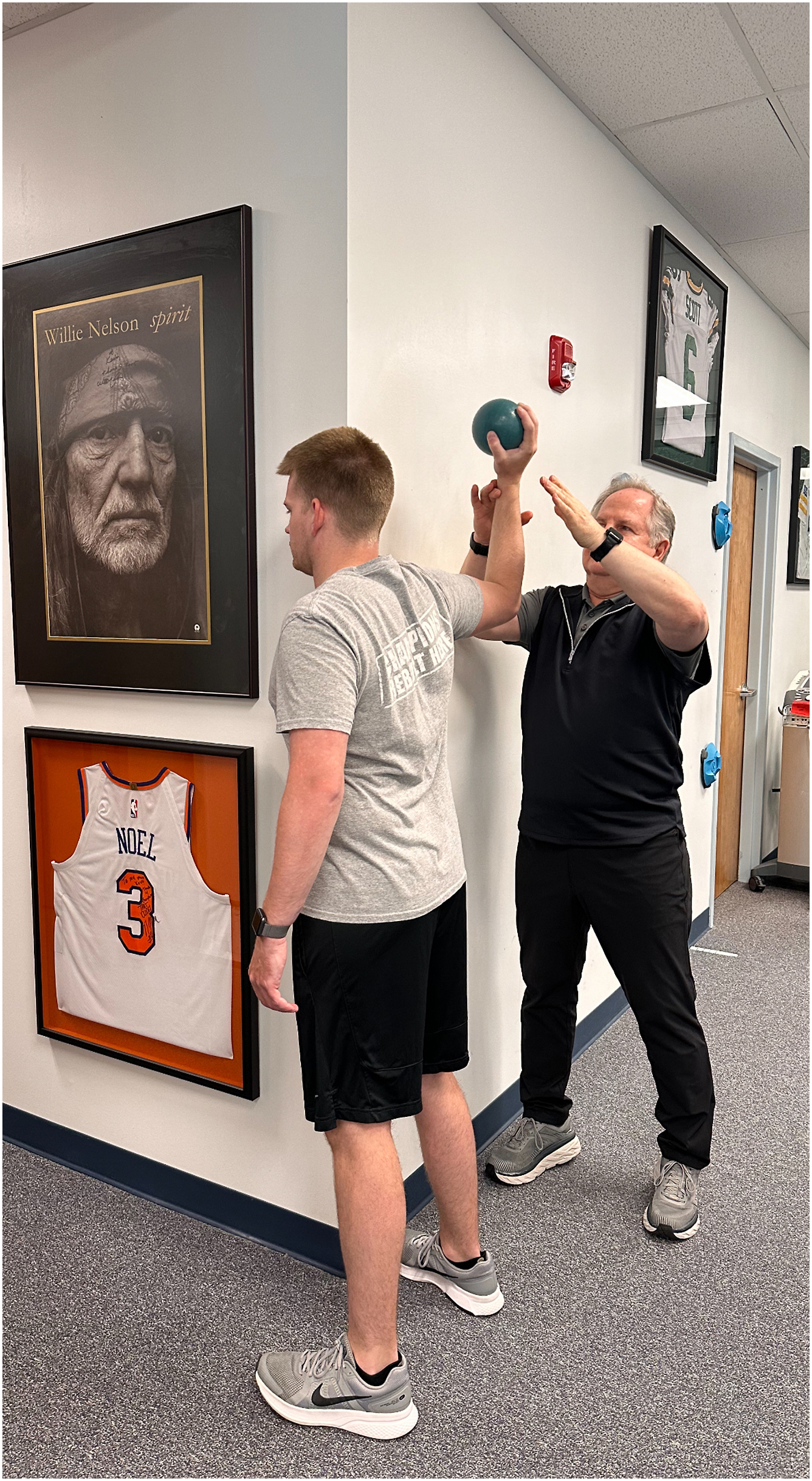
Closed kinetic chain exercises are advanced to include proprioceptive drills. This includes table push-ups on a ball or tilt board ( Fig. 5 ) as this has been shown to generate more upper and middle trapezius, and serratus anterior activity compared to performing a standard push-up exercise. Stabilization drills can also be performed with perturbations to the athlete’s arm while the hand is on a small ball ( Fig. 6 ).


Flexibility and ROM exercises for the shoulder and elbow joints are continued throughout this phase of treatment. The athlete will also integrate mobility, stabilization, and strengthening exercises for the trunk and lower back into the treatment program. In addition, athletes are encouraged to perform lower extremity strengthening and sport-specific conditioning activities beginning in this phase of the program.
Phase 3: Advanced Strengthening Phase
Phase 3 is designed to initiate aggressive strengthening exercises, augment power and endurance, progress functional drills, and gradually initiate throwing activities. Full shoulder and elbow ROM and flexibility should be maintained throughout this phase. Muscle fatigue has been shown to decrease neuromuscular control and diminish proprioceptive sense ; therefore, the athlete is challenged with strengthening activities used in the Advanced Throwers 10 program. This program incorporates challenging, alternating movement patterns focused on endurance to further challenge shoulder girdle neuromuscular control and facilitate activation of the rotator cuff musculature via alternating dynamic movements with sustained holds. The incorporation of sustained holds challenges the athlete to maintain a static position while the opposite extremity performs isotonic exercises. Three sets are incorporated into each exercise, each following a sequential progression integrating bilateral isotonic movement, unilateral isotonic movement with contralateral sustained hold, and alternating isotonic/sustained hold sequencing. The athlete can be instructed to perform these exercises on a stability ball to further challenge the core and postural control ( Fig. 7 ), as well as with manual resistance drills to increase muscle excitation and promote endurance of the upper quarter and core musculature.

Dynamic stabilization drills, such as RS performed in a functional throwing position, and ball throws are performed to improve proprioception and neuromuscular control of the throwing arm. Perturbations and end-range stability exercises such as RS while throwing a ball against a wall ( Fig. 8 ), push-ups onto an unstable surface with perturbations, and ER tubing with concomitant manual resistance are all utilized in advancing challenges to the athlete. In addition, these exercises can be performed on a physio ball to improve dynamic stabilization of the scapular, shoulder, arm, and trunk musculature. Advanced Throwers 10 exercises including prone horizontal abduction and row into ER with sustained holds and alternating arm/sustained hold sequencing are initiated to challenge the endurance of the posterior rotator cuff, scapular musculature, lumbar extensors, and gluteals ( Fig. 9 ). Side-lying ER, prone row, and prone horizontal abduction with manual resistance of the shoulder joint complex are utilized to promote increased muscular activity, neuromuscular control, and endurance, which are essential in the force production for overhead throwers.


Muscle fatigue has been shown to diminish proprioceptive sense, alter biomechanics, contribute to superior humeral head migration upon initiation of arm elevation, and increase valgus elbow stress. , , Kinematic and kinetic motion analysis performed by Murray and colleagues reported a decrease in shoulder ER ROM and ball velocity, along with lead knee flexion and shoulder adduction torque once a thrower became fatigued. Lyman and colleagues noted the greatest predisposing factor to shoulder and elbow injury in Little League pitchers was muscle fatigue. Based on these findings, muscle endurance training must be included in the rehabilitation program for overhead throwers. Endurance training includes wall dribbles with a Plyo ball (Functional Integrated Technologies, Watsonville, CA, USA), wall arm circles, upper body cycle, and Advanced Throwers 10 exercises.
Plyometrics are initiated to further enhance dynamic stability and proprioception while gradually increasing functional stresses on the upper extremity. The athlete is instructed to coordinate the trunk and lower extremity to efficiently allow the transfer of energy into the upper extremity during plyometric drills. Wilk and colleagues , have described a plyometric program that systematically introduces stresses upon the healing tissues, beginning with 2 handed drills such as chest pass, side-to-side throws, side throws, and overhead soccer throws. Upon successful completion, the athlete can progress to one-handed drills such as standing one-handed throws, wall dribbles, and plyometric step and throws ( Figs. 10–12 ).