Fig. 16.1
Prior to discontinuation/2 months later/7 months later/12 months later
Looking at the rash in the series of photographs 1, 2, 3 and 4 in Fig. 16.1, the dermatological diagnosis would clearly be AD. There is no obvious reason to consider the diagnosis of RSS. Photo 1 shows the patient shortly before discontinuing topical steroids where the rash was poorly controlled. Photo 2 was taken 2 months after ceasing topical steroids; photo 3, 7 months after cessation; and photo 4, 12 months after cessation. The patient did not make any lifestyle or environmental changes in those 12 months—all he did was stop the use of topical steroids. If his diagnosis was contact dermatitis secondary to the topical steroids used, then recovery should have been swift. His skin would not have gotten worse as it did—the severity of his symptoms actually peaked during the 2nd month before improving over the next few months. So, if you consider the rash at just one point in time, the diagnosis would almost certainly be AD. However, taking into account the history of topical steroid use and then cessation and the subsequent progression of the rash, the diagnosis of RSS is obvious.
It is easy to make a diagnosis of RSS when the patient’s symptoms are severe, as in the case shown in Fig. 16.2. Photograph 1 was taken just before the patient discontinued topical steroids. Here, the patient’s skin condition appears too severe to be a typical case of AD. In photo 2, taken 2 months after cessation of topical steroids, we see exudative erythema, incrustation, exfoliation, pigmentation and scars secondary to scratching. The patient developed a fever of around 40° which lasted 7–10 days and was thus suspected of having adrenal insufficiency. However, his blood cortisol levels were actually raised (not reduced).

Fig. 16.2
Prior to discontinuation/2 weeks later/3 months later/7 months later/13 months later
In some cases RSS progresses slowly after discontinuation of topical steroids. In these cases both the doctor and patient may become disheartened and doubtful whether management is appropriate. In Fig. 16.3 we see a case where symptoms peaked 7 months after ceasing topical steroids before gradually resolving.

Fig. 16.3
Prior to discontinuation/3 months later/7 months later/11 months later/19 months later
After ceasing topical steroids, a patient with RSS will develop extremely sensitive skin, and dermatitis will appear following exposure to even slight irritation. False positives are common in patch tests done around this time. Temporary exacerbations may result from seasonal changes such as changes in temperature and/or humidity or shedding of hair by pets. Unexpected flares can occur, for example, when a patient moves to a new location. Patients can thus experience a second or third rebound.
Therefore to determine whether a patient is heading towards recovery, the doctor needs to observe the patient for at least 12 months, ideally comparing skin status throughout the seasons over several years. For example, the patient in Fig. 16.3 can be assured of their improvement by comparing photos taken at 7 and 19 months after cessation of topical steroids.
16.2 Causes of RSS
Rapaport focussed on the vasodilation action of nitric oxide (NO) and suggested NO was a cause of RSS [6]. Cork proposed a theory that topical steroids increase protease, which breaks down corneodesmosome, which is in turn known to bind corneocytes to each other, and this is what breaks down the epidermal barrier leading to rebound symptoms [7].
In recent years it has been found that keratinocytes produce cortisol to autoregulate epidermal thickness and differentiation by paracrine and autocrine mechanisms [8]. The author believes that the long-term continuous use of topical steroids affects the cortisol production by keratinocytes, thereby causing RSS [9, 10].
Figure 16.4 shows the epidermal changes seen on the inside forearm of a healthy individual who had applied 0.05% clobetasol propionate twice daily to the area for 2 weeks before stopping. The images shown are of the skin before topical steroid use, day 2 of use, day 15 (i.e. 1 day after ceasing topical steroids) and day 30 (i.e. 16 days after stopping the topical steroid). Immunostaining for anti-PCNA antibodies, anti-cortisol antibodies, anti-11-beta-HSD1 antibodies and anti-11-beta-HSD2 antibodies is demonstrated. Atrophy to epidermis is evident on day 15, and on day 30 this atrophy was seen to be resolving. The intracytoplasmic cortisol in the keratinocytes peaked on day 15, showing the topical steroid use caused an increase in the cortisol production by the epidermis. This response has already been demonstrated in dermal fibroblasts [11]. It appears that the concentration of cortisol in the skin varies almost immediately in response to blood levels of cortisol (which are determined by the adrenal cortex).
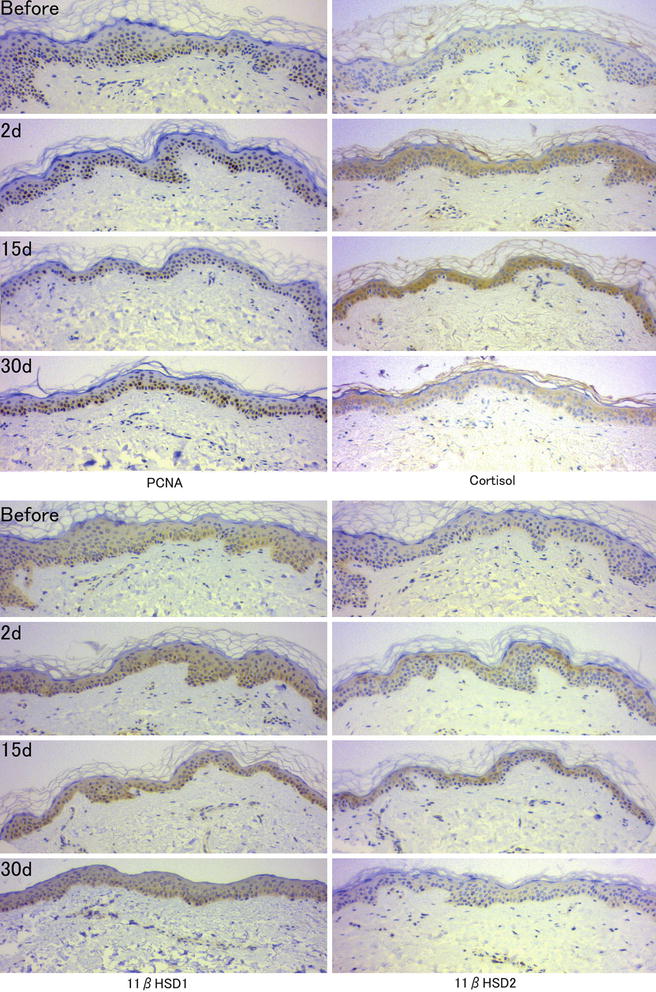
Fig. 16.4
The epidermal changes seen on the inside forearm of a healthy individual who had applied 0.05% clobetasol propionate twice daily to the area for 2 weeks before stopping
Intracytoplasmic cortisol and 11-beta-HSD2 both increase in keratinocytes. 11-Beta-HSD1 is an enzyme that converts cortisone, an inactive steroid, into cortisol, whilst 11-beta-HSD2 converts cortisol into cortisone. Therefore, increased levels of 11-beta-HSD2 indicate cortisol within the keratinocytes is being inactivated.
Figure 16.5 demonstrates a patient’s epidermis with immunostaining during RSS and during recovery 2 years later.
Fig. 16.5
A patient’s epidermis with immunostaining during RSS and during recovery 2 years later
The amount of 11-beta-HSD2 near the basal level is increased during RSS. In the recovered epidermis, 11-beta-HSD2 levels had reduced. The epidermal thickness has normalised, as has the granular layer, and the parakeratosis has disappeared. The evidence from this case suggests increased 11-beta-HSD2 in the epidermal basal layer is a cause of RSS. This means cortisol is inactivated to cortisone in the keratinocytes leading to increased proliferation of basal cells and immature keratinisation. This is explained in the diagram in Fig. 16.6.
Fig. 16.6
 Evolution and Development of Topical Corticosteroids
Topical Corticosteroid Addiction
Topical Side Effects of Topical Corticosteroids
Evolution and Development of Topical Corticosteroids
Topical Corticosteroid Addiction
Topical Side Effects of Topical Corticosteroids
 Dermatological Indications and Usage of Topical Corticosteroid
Dermatological Indications and Usage of Topical Corticosteroid
 Use and Misuse of Topical Corticosteroid in Genital Dermatosis
Use and Misuse of Topical Corticosteroid in Genital Dermatosis
 Topical Corticosteroid Abuse: Southeast Asia Perspective
Topical Corticosteroid Abuse: Southeast Asia Perspective




The first picture shows normal epidermis before application of topical steroids. The second shows increased cortisol levels and a thinner epidermis as a result of topical steroid application. The third picture shows the epidermis’s progression to topical steroid addiction with increased levels of 11-beta-HSD2 and the conversion of cortisol to the inactive cortisone. The fourth picture shows the epidermis of RSS with abnormal thickening and cortisol still being inactivated to cortisone
Related posts:
Evolution and Development of Topical Corticosteroids
Topical Corticosteroid Addiction
Topical Side Effects of Topical Corticosteroids
Dermatological Indications and Usage of Topical Corticosteroid
Use and Misuse of Topical Corticosteroid in Genital Dermatosis
Topical Corticosteroid Abuse: Southeast Asia Perspective
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
