Fig. 8.1
E.B, 45 years old, healthy BRCA2+, bilateral V-NSM with immediate one-step prosthesis reconstruction. a–b Preoperative frontal and lateral view. c–d Frontal and lateral view 9 months after intervention: cosmetic criticism due to asymmetry and insufficient fullness of reconstructed breast; ischemia of right nipple healed with lost of projection. e–f Frontal and lateral view 15 months after intervention and 6 months after lipoaspirate injection (2 procedures) and repositioning of the left prosthesis: volume, shape, and symmetry are excellent now. Right nipple lost will be reconstructed with local dermal flaps

Fig. 8.2
GB, 41 years old, sister of EB, right radical mastectomy for BRCA2-associated breast cancer, followed by left prophylactic contralateral simple mastectomy. Two years after intervention, expander-prosthesis and nipple-areola reconstruction. Although if cosmetic outcome is very good, the scar and a reconstructed NAC as well as the breast shape make the result less beautiful as compared as the final result of her sister’s MM, showing the potential cosmetic superiority of the latter technique, even when complications underwent
It should be pointed out that SSM and NSM techniques, performed either for early cancers or RRS, are the ones procedures which require per se immediate reconstruction, since the skin/NAC saved have to be “filled” in order to avoid tissue retraction, thus loosing the shape of the breast skin envelope given by the techniques themselves along with the chance of the best possible esthetic outcome. Several methods of reconstruction such as autologous flaps, tissue expanders, biologic mesh with fat injection or one-step prosthesis positioning have been described. Which of these methods should lead to the best results, as well as more or less nipple loss or additional morbidity, remains unknown and comparative studies are needed.
Implant-based reconstruction is the preferred technique by most Authors for conservative mastectomies [5]. Except for skin reducing-NSM (SRM), which was ideated to be performed with definitive prosthesis reconstruction, a two-stage technique is mainly performed. The two-stage method means to undergo the subsequent steps: first, insertion of an expander behind the pectoralis muscle; then, its progressively inflation which provides a progressive distention of the teguments and a more natural shape; finally, the second step surgery, when the expander is substituted by an anatomically shaped definitive silicon prosthesis. The technique usually requires a contralateral plastic surgery to reach symmetry.
A multistep reconstruction allows for NSM optimal cosmetic results, including “second look” refinements such as a perfectly defined inframammary fold, the precise position of reconstructed NAC, the possibility for contralateral augmentation to reach symmetry (sometimes a need of surgeon rather than patients’ request, since the positioning of contralateral prosthesis may improve to reach symmetry with the reconstructed breast).
However, immediate definitive reconstruction after CM is strong appealing for women since it reduces the need for multiple postoperative office visits and subsequent surgery. Although if this is the rule in SRM as a part of the technique, it is infrequently choosed after SSM/NSM. This is mainly due to the advantage given by the expander of avoidance retroareolar pressure in the immediate postoperative days, when the areola is at risk of ischemic damages, as well as to protect viability of skin flap by eliminating any tension [12, 13]; furthermore, a volume-fixed prosthesis under major pectoralis muscle is either not always feasible or results in a low projection of the lower pole of the breast. Nonetheless, immediate definitive reconstruction with a permanent anatomically shaped prosthesis has been successfully described by several authors both with conventional technique of subpectoral pocket [14] and with the new aid of human acellular dermal matrix for the lower pole coverage [15, 16].
8.2 Reconstruction After Minimally Invasive Mastectomies: Work in Progress Rather than State-of-the-Art
Until now, video-assisted BCS and minimally invasive mastectomies (MM) have been performed as innovative experiences in few series. Here we focus only on MM, which is strictly the theme of this book. First experiences from Japan and China reported on endoscopic subcutaneous mastectomy are mainly performed together with immediate prosthesis reconstruction except for Nakajima et al., who used the latissimus dorsi muscle flap [17–23]. All these Authors underline the advantage of the video-assisted technique for cosmetic outcome, since the procedure results in minimal scarring and restoration of breast volume. However, methods used for reporting satisfaction with the cosmetic result are strongly heterogeneous and usually come from a subjective prospective, thus failing until now to definitively demonstrate a superior cosmetic advantage as compared with traditional open technique [24, 25].
Kitamura [17] and Fan [23] employ more objective methods including self satisfaction indices and doctors’ rating scales (0–3 = poor–excellent); although they could not demonstrate a statistical difference in patient’s self-reporting of cosmetic outcomes, Kitamura [17] was the first author who reported a trend toward superior cosmetic outcome following endoscopic subcutaneous mastectomy (85.6 % “excellent outcomes” as compared to 60.0 % after open SM). On the contrary, Fan et al. [23] observed a low (20.9 %) rate of “excellent results”, although if it was comparable to the cosmetic outcome of patients treated with conventional surgery; however, acceptable satisfaction (excellent + good + fair) was achieved in 88.4 % of cases. Unfortunately, they compared endoscopic SM with BCS rather than open SM, which is, in authors’ reviewers [24, 25] as well as in ourselves point of view, inappropriate.
All these reports on MM belong to the “subcutaneous mastectomy (SM) era”. In fact, before the last 10 years, SM has been seldom used by few breast surgeons since it has never been considered in guidelines as an adequate procedure from an oncological point of view, due to the variable amount of tissue leaved under the NAC. Nowadays SM has been replaced by the NSM, a new revolutionary concept of conservative mastectomy already accepted as oncologically safe and widely taken into clinical practice for selected indications [5, 25, 26], even if in absence of level I evidence from randomized trials [28].
Now the “NSM era” that has started MM should means video-assisted NSM, performed with the same technical skills required for open-NSM, aimed to the total glandectomy including the radical dissection of the NAC and immediate reconstruction.
The unique reports on endoscopic NSM come again from Asia by Sakamoto et al. [29] and for the first time from an Occidental country, Italy, by the authors of this book [30]. Breast reconstruction after such a procedure is then at its earliest experience phase: the issue of the dissected NAC was not assumed in previous procedures of endoscopic SM, so that we must be aware that more extensive experience is needed to assess a “stated of art” (interestingly, we should remember that the same issue is still on debate in open NSM itself) of reconstructive options in MM.
Surprisingly Sakamoto et al.’s “rarely” underwent immediate reconstruction, although they anticipate an ongoing experience with prosthesis reconstructions under endoscopic assistance [29]; a series lacking of reconstruction step misses maybe the strongest motivation to undergo MM, which is a cosmetic improvement and patients’ better quality of life by avoiding scars on the breast; furthermore, reconstruction procedures affect both complication rates and cosmetic outcome, so that results of this series, when available, should be evaluated taken into account this initial bias [31]. As a result, the sole early experience available of breast reconstruction after V-NSM is the one of the authors of this book. Most of our patients underwent an endoscopic-assisted immediate reconstruction with positioning of an anatomically shaped, definitive prosthesis under the major pectoralis muscle [30]. Complications related to reconstruction in ous series were: three cases of implant migration, only in one case associated with reversible ischemia of NAC/skin-flap, requiring prosthesis removal (2.5 %); one capsular contraction after prolonged lymphorrhea (total morbidity 10 %). Case of prosthesis infection was not seen. In 40 % patients good/excellent symmetry could be achieved just after one step surgical procedure (Fig. 8.3); in the remaining 60 % of cases, further procedure such as lipoaspirate injection and/or mild contralateral pexis, as well as three cases of contralateral augmentation (Fig. 8.4) have been either to reach a better symmetry or for woman’s desire. Early and medium (1 year) time cosmetic outcome was either good or excellent in 90 % of cases both for patients and surgeons’ point of view, as measured by a rating 0–10 scale (good = 7–8; excellent = 9–10).

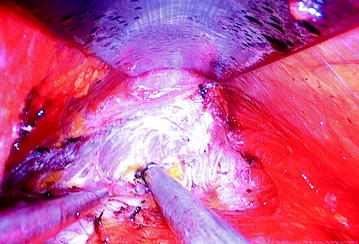
Fig. 8.3
Patients’ cosmetic oucome after one-stage prosthesis reconstruction with no need for further plastic procedures. a R.S., 47 years old, 2 years after left V-NSM for BC; b R. I., 43 years old, 6 months after left V-NSM for BC. The medium anterior thoracic scar is due to a previous cardiosurgery procedure; c O.C., 54 years old, 10 months after dx V-NSM for BC. d GF. B., 54 years old, 5 months after right V-NSM for BC; lipoaspirate injection was proposed to optimize the lower pole, but the patient did not feel the need
Fig. 8.4
Videoscope imaging during the preparation of a submuscular pocket for immediate reconstruction. Here it can be observed as the achievement of the subfascial yellow fat after detachment of the insertions of muscle pectoralis major, at sternal aspect and inframammary fold. Magnificated details allow to recognize structures obtaining an excellent surgical control
Assuming that these data are from a very early and investigational experience with a totally new technique both of mastectomy and of breast reconstruction, improvements are expected in the next years, although at present several trick and pitfalls regarding reconstructive step have been already observed and reported in the next paragraphs.
8.3 Total Submuscular Prosthesis Position
In the field of breast esthetic surgery, the use of silicone gel breast implants via axillary route for breast augmentation have been employed as alternative to avoid direct skin-breast accesses from many years; however, it has been only with the aid of endoscopic assistance, proposed by Price et al. [32] in 1994, that transaxillary route became more popular among plastic surgeons since video-assisted technique allowed for direct tissue visualization and provided an improved level of technical control [33, 34] previously unseen with the blind approach.
The transaxillary access for breast augmentation has a certain appeal for both patients and surgeons, in that it allows placement of the implant through a remote incision, thereby limiting obvious postoperative scarring. Although if some concerns have raised regarding the risks of implant damage with remote incision sites, endoscopic-assisted breast augmentation with transaxillary approach has already become a reasonable safe option allowing excellent cosmetic outcome [35]. Due to these validated experiences in the field of esthetic surgery, when minimally invasive approach was applied to the breast oncologic surgery, a reconstruction through transaxillary approach after MM could start with awareness of such a background, even if applied in a different setting implying totally different technical demands.
Immediate, usually one-stage, prosthesis reconstruction, has been until now the preferred technique of breast reconstruction after MM (Table 8.1), since only Nakajima et al. used the latissimus dorsi flap [18] reporting no major morbidity and satisfactory esthetic results.
Table 8.1
A summary of the most relevant casuistic of V-NSM referred to the reconstruction procedure associated
Years | Author | N. | Ind. | BS | Incision | REC option | REC morbidity | Good cosmetic outcome % |
|---|---|---|---|---|---|---|---|---|
2002 | Kitamura et al. | 21 | BC | SM | Axilla 6 cm | Saline-filled P | 4.8 % | 90.4 % |
2002 | Nakajima et al. | 17 | BC | SM, AD | Axilla 5–7 cm | LD flap | None | 100 % |
2002 | Ho et al. | 9 | BC | SM, AD | Axilla 5–7 cm ± Areola | Expander | None | 100 % |
2006 | Yamashita and Shimizu | 2 | DCIS | SM | Lateral chest 5 cm | 1 none 1P | Ne | Ne |
2008 | Ito et al. | 33 | BC | SM, SNB ± AD | Axilla 5 cm + B skin | P | 9 % P removed for infection 3 % contraction | Yes (78.8 %?) |
2008 | Yamaguchi et al. | 21 | BC | SM | Axilla 8 cm or IMF | Rec | Ne | Ne |
2009 | Fan et al. | 43 | BC | SM, AD | 3 B skin/ axilla 0,5 cm | P | None | 58.1 % (88.4 %) |
2009 | Sakomoto et al. | 89 | BC | NSM, SNB, ± AD | Axilla 3–5 cm and Areola ± Nipple | Few P | No data | Ne |
2012 | Ferrari A, Sgarella A, Zonta S | 40 | BC, RRS | NSM, SNB ± AD | 3–4 cm Axilla | P-rec | X % 2 P migration 1 P contraction | 90 % |
Kitamura et al. used a saline-filled prosthesis placed into a submuscular pocket which was performed under endoscopic guidance with the same criteria used in open technique [17]. Interestingly, complications observed were significantly less common in patients treated with endoscopic SM rather than with conventional SM (4.8 % versus 12 %; P = 0.4).
The creation of a subpectoral pocket by the aid of the harmonic scalpel under endoscopic vision represented the first surgical step in the procedure described by Ho and coll, before MM itself. This subpectoral space performed down to a level 1 cm caudal to the inframammary fold was used for the insertion of an expander later on, after SM and axillary surgery had underwent [19]. The authors do not give information on second-step surgery, even if they report excellent results in all 9 patients of their study.
Yamashita and Shimizu report mainly on endoscopic BCS, even if it means in several cases a partial or subtotal mastectomy (33–50 % or even more than 50 % of breast tissue excision). Interestingly, they used absorbable fiber mesh or cotton to fill the defective part of the gland after these extensive breast resections [36]. However, only two anecdotical cases of endoscopic SM were reported, one without reconstruction, the other one with immediate prosthesis reconstruction [20]. Ito and coll. reported a series of 30 immediate breast reconstruction after 33 video-assisted SM: the pocket beneath the pectoralis major muscle was created bluntly, and a definitive mammary prosthesis was then inserted inside [21]. Cosmetic results have been subjectively evaluated as excellent, however, this should be not true at least in three cases: three without reconstruction, three who underwent prosthesis removal due to infection and 1 who developed capsular contraction (12 % morbility strictly related with reconstruction). So it can be extrapolated that the reported excellent cosmetic results are referred to 26 out of 33 patients (78.8 %).
Immediate reconstruction with a definitive prosthesis is the technique used also by Yamaguchi et al. [22], but no further data are available on specific outcome.
Fan et al. experience concludes the Oriental reports of MM intended as endoscopic-assisted SM (with author’s word: “a small amount of the gland has been spared beneath the nipple and areola to prevent ischemia and aversion”: which is the key critical issue that makes the difference between SM and the new concept of NSM) [23]. Again, breast reconstruction was performed with “a suitable prosthesis of 180–260 ml that exactly matched the volume of the excised gland and the contralateral breast placed into the retropectoral space”; it was not specified if the pocket was performed under endoscopic guidance or not, so maybe it was not. No reconstruction-related complications are reported, and a satisfactory cosmetic result (excellent/good) was achieved in 58.1 %; 88.4 % if fair results were included.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


