Fig. 9.1
First V-NSM we performed in Pavia, Italy. Technique with the aid of a retractor. a–b the èquipe during intervention follows dissection of the breast under the guidance of a video camera, c the detail of the axillary access with the retractor and operative instruments inside, d at the end of the procedure
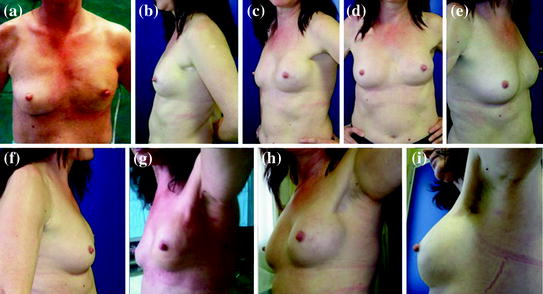
Fig. 9.2
a Early postoperative outcome after left V-NSM. Uneventful postoperative course: The drainage (was removed and the patient was discharged on 4th postoperative day. b–f Late postoperative outcome after left V-NSM. From right lateral to left lateral view, the symmetry is excellent without any further plastic procedure. g–i: Axillary scar. Evolution of the scar after 1 month (2 h), 3 months (2i) and 2 years 2(l), when 24 months after V-NSM the scar has become almost invisible
The oncological follow-up of this patient is only 2 years long, however, very interesting. The family history of the woman was positive even if not paradigmatic for hereditary cancer (her maternal uncle and grandmother had breast cancer at 50 years booths). After clinical and genetic counselling, she underwent genetic test for a BRCA 1-2 deleterious mutation. A BRCA1 mutation of unknown clinical relevance according to Breast Cancer Database was found (exon 16: Met1652IIe). Interestingly, one-year after patient’s cancer, the mother of herself developed breast cancer too. After this event patient’s pedigree became suggestive for hereditary cancer, and the same BRCA1 mutation of unknown clinical relevance was found also in the mother’s genetic test. The patient remained on stage IV NED (no evidence of disease) for 18 months after surgery, when a solitary subcutaneous metastasis was detected close to the scar of orthopedic intervention on fractured humerus for bone metastasis at presentation of disease. Re-staging with CT-PET showed further three vascularized lesions, smaller than 2 cm in size, under the right pectoralis muscle. No local recurrence was detected in the site of left V-NSM. A core biopsy of the nodules confirmed a distant recurrence of breast carcinoma, mucinous type, G2, ER 95 % PgR 1–2 %, Ki-67 7 %. After MDM discussion, the patient underwent a first-line chemotherapy treatment with anthracyclines and taxanes, which is presently ongoing.
9.3 Case No. 2 E.B., 45 Years old. Bilateral V-NSM for Risk Reduction: Nipple Lost
G.B., a 41-year-old-woman and a doctor herself, was treated for breast cancer in our breast unit. Due to her positive family history, she underwent genetic counselling and BRCA test. A deleterious BRCA2 mutation was found, and the doctor/patient decided for a contralateral prophylactic simple mastectomy and salpingo-oophorectomy. In the meanwhile, her two sisters made genetic test, both resulting positive for the same BRCA2 mutation. These three sisters lost their mother in their teens age, and the disease had already developed in one of them: these facts deeply shocked also the healthy ones. Psychologic support was offered, and genetic and clinical post-test counselling was made during 12 months. Such long time was necessary to overcome the distress thus allowing decision-making with awareness and serenity. Their final choices were: one sister opted for surveillance, the other one for risk reduction breast surgery, waiting for an isteroannessiectomy to perform later on. Since we had already started the clinical program of minimally invasive NSM, the woman who chose risk reduction surgery (RRS) was exhaustively informed on lights and shadows of the innovative procedure and about the absence of codified indications of minimally invasive mastectomies (MM) for RRS, even though there was already an increasing body of evidence in the literature, at least on conventional NSM; after discussion, she opted for the new technique.
E.B., 45 years, was indeed the first healthy woman who underwent bilateral V-NSM for risk reduction. She had medium-size, mild ptotic breasts, which represented a very important part of her feminine body image and beauty (Fig. 9.3a–b). Bilateral V-NSM was performed in double èquipe. Postoperative course was uneventful for major complication, but a right nipple ischemia developed resulting in the lost of nipple projection and mild discoloration of the areola. Furthermore, surgeons and patient’s late satisfaction for cosmetic result was low due to a lateral dislocation of the left prosthesis, causing poor symmetry and loss of fullness of décolleté (Fig. 9.3c–d). Preoperative breast appearance was very beautiful and a similar original size and softness was difficult to reach through a one-step surgical approach. A dual-phase reconstruction with the use of an expander would have been a good, maybe better, alternative choice. However, she underwent a second operation: though the same axillary scars both prosthesis were easily substituted with greater size ones, while providing the correction of the left implant dislocation; at the same time, a lipoaspirate injection provided a natural look and softness to the reconstructed breasts, while optimizing symmetry. Final cosmetic result after the minimally invasive “second look” plastic operation was excellent, both from the patient’s and her doctors’ point of view (Fig. 9.3e–f). Two years after RRS, the woman is healthy and has not overcome any psychological distress.
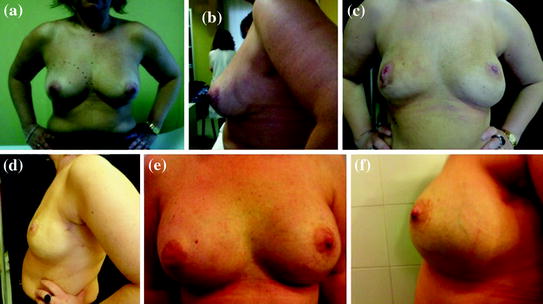
Fig. 9.3
a–b a 45-year-old BRCA2-positive healthy woman asking for risk reduction surgery; c–d 3 months after bilateral MM: ischemic loss of the right nipple and low cosmetic satisfaction due to left implant dislocation, suboptimal prosthesis volume, asymmetry, and “empty” breast shape; e–f 1-year after: plastic intervention through axillary scars was performed, including implant substitution with a bigger size prosthesis and lipofilling procedure, thus correcting cosmetic criticism and obtaining a satisfactory result
9.4 Case No. 3 L.G. 38 Years old. An Other History of RRS
Eighteen months ago L. G., a 36-year-old-woman, came to our risk clinic due to her new awareness of the problem after our breast unit made a popular scientific conference in her town on breast cancer, giving information’s on familiar risk. Her personal medical history was positive for endometriosis. Her family history was strongly positive for breast cancer: her mother at 40 year, maternal uncle at 38 year, maternal cousin at 28 year, paternal uncle at 45 year.
Since she had no relationship with her young cousin, who was the one survivor, she underwent clinical and genetic counselling and then genetic test searching for a BRCA1/2 mutation. The test was made with public health service and the result came after 12 months. In the meanwhile, she started a surveillance program. She underwent a breast magnetic resonance, which found no tumor in her breasts, and periodic gynecologic visits. Finally, she had the result of her genetic test, which demonstrated a deleterious BRCA 1 mutation. The woman had a genetic and clinical post-test counselling, and decided to continue the surveillance program while thinking about RRS option. During a gynecologic control, on transvaginal ultrasound, an hyperplastic endometrium with a maximum thickness of 13 mm was detected. Further examination included tumor markers on blood samples, with Ca 125:50, 9 U/ml in accordance with the previous diagnosis of endometriosis, and a sonohysterography which revealed a polypoid endometrium. Then the patient underwent a diagnostic hysteroscopy with pathologic exam on endometrial biopsies, showing atypical complex glandular hyperplasia and endometrial adenocarcinoma G1. So, an asymptomatic endometrial carcinoma was diagnosed after 18 months from her first access to the risk clinic. The patient underwent a hysterectomy and prophylactic bilateral salpingo-oophorectomy. Pathologic exam demonstrated an intramucosal endometrial adenocarcinoma 10 mm in diameter, G1, stage IA; ovarian endometriosis was found in each ovary. Since the early diagnosis of the tumor, adjuvant therapy was not indicated.
The woman was already under psychological support, and had time to think about breast RRS. After treatment of endometrial tumor, she asked for prophylactic bilateral mastectomy.
At 38 years, 24 months after her first access to our risk clinic, she underwent bilateral nipple sparing mastectomy through minimally invasive, endoscopic-assisted technique. Immediate reconstruction was performed with a definitive, silicon anatomically shaped implant. Postoperative course was uneventful and early outcome was excellent, with skin/nipple optimal viability, and a very good symmetry (Fig. 9.4).
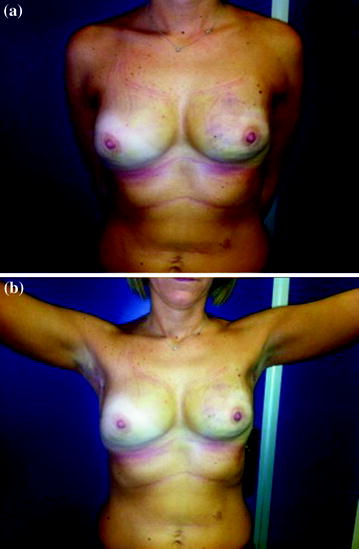
Fig. 9.4
Early postoperative outcome 1 month after bilateral V-NSM for RRS in a healthy BRCA1-positive 38-year-old woman. NAC and skin viability, as well as symmetry after one-step immediate reconstruction are excellent (a) and scars are well-hidden in axilla (b)
9.5 Case No. 4 R.M., 33 Years old. First BESS Technique for Breast Cancer. Postoperative Bleeding
R.M., 33 years, came to our breast unit since she felt a nodule in her right breast, which was confirmed at physic exam. Diagnostic workout included mammography, which demonstrated a plurifocal area of microcalcifications (60 mm large as a whole) suspicious for carcinoma, in the outer and central quadrants of the breast; ultrasonography showed ductal ectasia, microcalcifications, and also a 5-mm ipoechoic area of doubtful meaning. A vacuum-assisted aspiration breast biopsy was performed, and pathologic exam demonstrated an intraductal neoplasia DIN2-DIN3, ER 90 %, PgR 80 %, Ki-67 15-20 %, C-erb B2 ++. A breast NMR was also performed to obtain a better local staging of this multicentric disease in a young woman; the exam confirmed a large neoplastic involvement of the right breast, no suspicious lymph nodes, no contralateral lesions. Patient’s breasts were small and grade 1 ptotic. MM was proposed with a brand new technique, unique worldwide, which we had developed and were going to apply for the first time: breast endoscopic surgery with single-site (BESS) access, and low CO2 flow to obtain the working space (Fig. 9.5a). The technique is described in this book as well as in the Literature [3, 5].

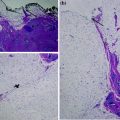
Fig. 9.5
First worldwide BESS procedure for MM, obtained with the aid of a single-port device and CO2 flow (a). On 3rd postoperative day after reintervention for bleeding: the hemostasis was obtained through the minimally invasive access, without the need to “open” the breast skin (b–c). Late (14 months) outcome, d–f good cosmetic result despite of postoperative complication and one-step definitive reconstruction
On first postoperative day, an hemorragic compliance developed. It appeared both as hematoma in the submuscular space, causing breast swelling, and active bleeding into the drainage. The patient underwent emergency surgery to obtain hemostasis. Interestingly, the procedure was performed without need to open minimally invasive access unless enlarging the scar for about 2 cm. The prosthesis was removed and endoscopic-assisted hemostasis was obtained with the aid of a Ligasure scalpel inside the pocket, guided by video-imaging. After rapid control of bleeding, which came from sternal aspect of the pocket, the prosthesis was reinserted inside and the pocket closed. Subsequent postoperative course was uneventful.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


