Reconstruction of the Lips
Introduction
The upper and lower lips compose a distinct anatomic unit that is the principal feature of the lower face. The lips have a major importance to facial appearance and function. Reconstruction of the lip can present a challenge to the reconstructive surgeon who seeks excellence in restoration of the aesthetics and functioning of this unique structure. Descriptions of lip reconstruction date to at least BC 1000 in the Eastern Sanskrit writings of Susruta.1,2 Early reports of lip reconstruction in the Western literature date to at least the first century (Fig. 19-1). Description of the classic V-shaped excision of the lip and primary repair has been credited to a writing by Louis in 1768, although this method of treating lip neoplasms was certainly performed many centuries before that.1 A large variety of methods for reconstructing the lips were developed and reported in the medical literature of the 19th century, from which most of the procedures performed today have some derivation.
Anatomic Considerations
Lip tissue is a composite of skin, muscle, and mucosa (Fig. 19-2). The most distinguishing feature of the lip is the vermilion, which is modified mucosa that covers the free margin of the lips and is adapted for external exposure. There are relatively few glands beneath the vermilion, in contrast to the multitude of minor salivary glands found immediately deep to labial and buccal mucosa. The well-defined line where the anterior limit of the vermilion adjoins the adjacent lip skin is referred to as the mucocutaneous or anterior vermilion line. It represents an important landmark in lip reconstruction. The posterior vermilion line is defined as the innermost line of contact between the upper and lower lips when the mouth is closed. Labial vermilion is characteristically red among those of light skin color and dark among those with dark skin color. Fullness of the rounded vermilion, particularly in women, is considered a mark of beauty in many cultures.

Upper and lower labial arteries are the principal vascular supply to the lips. Both arteries are derived from the facial artery on either side of the face. The labial arteries course horizontally across the lip in the submucosal plane, immediately posterior to the orbicularis muscle at approximately the same level as the anterior vermilion line. Whereas the labial artery of the lower lip tends to remain in the same horizontal plane as it crosses the lip, that of the upper lip may rise slightly as it passes medially toward the center of the lip. Some labial arteries may have a tortuous course through the muscle. The course of the labial artery can be detected with gentle palpation and is typically easy to map out with use of a Doppler device. In studies of arterial anatomy of the lower face, a variable pattern of vessels anastomosing across the lower lip and chin was found, with one or more vertically oriented labiomental branches descending to the chin region. A horizontally oriented mental branch was noted in many cases.3,4 Multiple anastomoses between the vertical and horizontal branches were observed when both were present.3 In the central region of the upper lip, the superior labial artery gives rise to multiple septal and alar branches.3 The exact pattern for venous drainage is less well defined and has commonly been considered to be largely by venae comitantes. Superior and inferior labial veins have been described. Both veins typically drain into the ipsilateral facial vein and are less distinct than the arteries and difficult to identify. In a cadaver study, Park et al3 identified a deep venous system of the upper lip that was considered to be independent of the arterial system. An understanding of the vascular supply of the lips is important in the planning of many reconstructive lip flaps.
The limit of the superior border of the upper lip centrally is the nasal base. The limit of the inferior border of the lower lip centrally is the mental crease, which separates the lip from the chin. The lateral borders of the upper and lower lips are marked by the melolabial and labiomandibular creases that separate the lips from the cheeks. These peripheral defining lines may not be so obvious in young children, but they are more pronounced with age and are recognized natural lines of the face. The melolabial and mental creases mark the sites where muscles of facial expression attach to the orbicularis muscle, providing the muscle with an indirect connection to the facial skeleton. These crease lines are strongly favored sites for making incisions required for excision of lip tumors and for the outline of many reconstructive flaps.
The relaxed skin tension lines for the lips course in a radiant fashion about the oral stoma in a manner analogous to the spokes of a wheel and reflect the wrinkle lines of older patients (Fig. 19-3). These lines are vertical in the central region of the lips and are progressively more oblique or slanted in lateral regions of the lips. The orientation of the lines is perpendicular to the underlying orbicularis muscle fibers. The philtrum is an embryologically derived structure with two parallel raised ridges that has no functional significance but has aesthetic importance to the central region of the upper lip. Incisions of either lip create less unsightly scars when they are made parallel to the long axis of the philtrum or to the labial relaxed skin tension lines.

FIGURE 19-3 Aesthetic borders of lips marked by melolabial and labiomandibular creases on either side and mental crease inferiorly. Rhytids of lips parallel relaxed skin tension lines, which display radiant pattern about oral stoma.
The lips exhibit multiple motor functions, which include various facial expressions, oral retention of food and liquids, articulation of speech, and the acts of whistling and kissing. The lips also have important sensory functions of touch, pain, and temperature perception, which enable the monitoring of materials that enter the mouth and provide some pleasures. The most ideal lip reconstructions are those that best preserve or restore these different functions. Restoration of the orbicularis muscle sphincter is highly desirable, particularly of the lower lip. As a general rule, it is best if reconstruction of the lip is accomplished from within the lip complex, except when that would result in excessive microstomia. In most cases, reconstruction of slightly more than half of either lip can be accomplished by use of tissue from within the respective aesthetic region of the lips. When additional tissue is required, most reconstructions involve the use of local flaps harvested from the adjacent regions of the cheek or chin. With current designs, any flap harvested from outside the lip complex to repair full-thickness lip defects fails to restore a complete functional orbicularis muscle sphincter. To a limited degree, tightness in a reconstructed lip may help compensate for deficiency of the muscle sphincter.
Vermilion Reconstruction
Mucosal Advancement Flaps
The most favored method of restoration of the vermilion is anterior advancement of the mucosa that lines the inner surface of the lip (Fig. 19-4). A mucosal flap is created by undermining beneath the labial mucosa in a plane that is deep to the minor salivary glands and superficial to the posterior surface of the orbicularis oris. If necessary, dissection may extend the entire vertical height of the lip to the apex of the gingivolabial sulcus. The flap is advanced forward over the free margin of the lip to the desired point, which is usually the anterior vermilion line. Because the vermilion is actually a modified mucosal surface, reconstruction with labial mucosa offers a close substitute. In most cases, a slight prominence of the soft tissue at the mucocutaneous junction is considered to be a favorable feature of lip contour. However, it is difficult to restore this fullness in areas reconstructed by mucosal advancement flaps. This may be related to contraction of the mucosal flap as the wound heals. There is less flap retraction when dissection of the flap requires limited undermining of the mucosa of the lip.

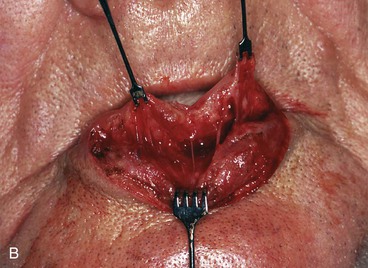
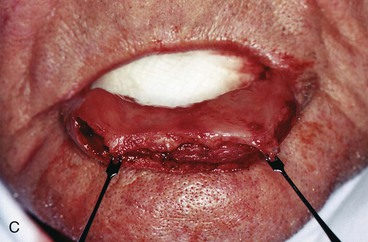

FIGURE 19-4 A, A 4 × 1-cm defect of lower lip vermilion and skin. B, Labial mucosal advancement flap dissected deep to minor salivary glands and immediately superficial to orbicularis muscle. C, Flap advanced. Margin of skin defect not dissected. Skin margin left to migrate cephalically by scar contraction. D, Anterior vermilion line in acceptable position. Continued scar maturation will reduce scar thickness.
Reconstruction of the vermilion with a mucosal advancement flap may produce a pleasing aesthetic restoration of either lip. However, several difficulties may be encountered with this technique. An early difficulty is restoration of accurate positioning of the anterior vermilion line when there is an adjacent skin defect at the lip margin. In such instances, wound contraction inherent to wound maturation may influence the position of the vermilion line. If distortion or displacement of the anterior vermilion line occurs, repositioning of the reconstructed line may be possible with revision surgery. Another difficulty encountered with mucosal advancement flaps is that the flaps tend to display a slightly deeper red color than that of the natural vermilion, especially in those with more “weathered” lips. In some cases, the darker red color can impart a slightly feminine appearance to the reconstructed vermilion, particularly when the flap covers a large surface area (Fig. 19-5).
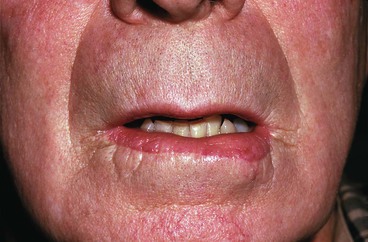
FIGURE 19-5 Mucosal advancement flap used to reconstruct inferior vermilion. Color is darker red than natural vermilion.
Whereas a majority of patients regain some degree of touch, pain, and temperature sensation to the reconstructed vermilion within a matter of several months after the employment of mucosal advancement flaps, there are individuals in whom sensory return is inadequate. Influenced by Karapandzic’s concept of lip flap design, this author performs dissections with a selective spreading technique in an attempt to preserve the small neural and vascular structures that are encountered as the mucosal advancement flap is dissected (see Fig. 19-4B).1,5,6 These neurovascular structures are then gently stretched forward with advancement of the mucosal flap.
Mucosal V-Y Island Advancement Flaps
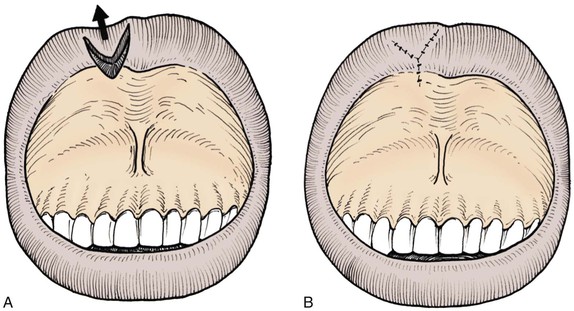
In some cases, small volume deficiencies of the vermilion may be restored with V-Y advancement flaps of labial or buccal mucosa (Fig. 19-6). The advancement flap is created by a V-shaped incision with the apex of the incision positioned toward the gingivolabial sulcus. Mucosal V-Y advancement flaps may also be created as island flaps to repair small adjacent vermilion defects. Incisions are made to the level of the orbicularis oris, creating an island flap that is pedicled on the underlying deep tissue. The triangle-shaped island is advanced into the adjacent recipient site, maintaining sufficient deep tissue attachments to ensure its viability. The donor site is closed primarily by direct approximation of the adjacent wound margins, resulting in a Y configuration to the wound closure. Closure of the donor site assists with securing the position of the advancement flap. Most V-Y island advancement flaps of the lip are designed to advance in a vertical or near-vertical orientation. There are some cases in which horizontal tissue movement is employed, with use of either a single island flap or bilateral opposing island flaps. Mucosal V-Y island advancement flaps are best suited for repair of small defects of the vermilion.
Mucosal Cross-Lip Flaps
A vermilion defect may in some cases be restored with an interpolated cross-lip transfer of labial mucosa or vermilion along with some underlying soft tissue (Fig. 19-7). Cross-lip transfer may be accomplished with a single-pedicle flap for small defects or a bipedicle flap (“bucket handle”) for wider defects that extend horizontally across the lip (Fig. 19-8). A cross-lip mucosal flap is typically designed as a linear band of mucosa, harvested from the region immediately posterior to the posterior vermilion line of the donor lip. The width of the band is determined by the width of the vermilion defect and by what will allow donor site wound closure. The mucosal flap is most often elevated in the plane immediately superficial to the orbicularis muscle, although some muscle may be included in the flap when it is necessary to fill a soft tissue defect of the recipient lip. The labial artery may be incorporated into larger flaps, providing an axial circulation and ensuring a greater likelihood of flap viability. Once it is dissected, the flap is transferred across the oral aperture to the vermilion defect and sutured in place (Fig. 19-9). The donor site is closed primarily. Division of the pedicle and flap inset are performed 3 weeks later as a second-stage procedure.
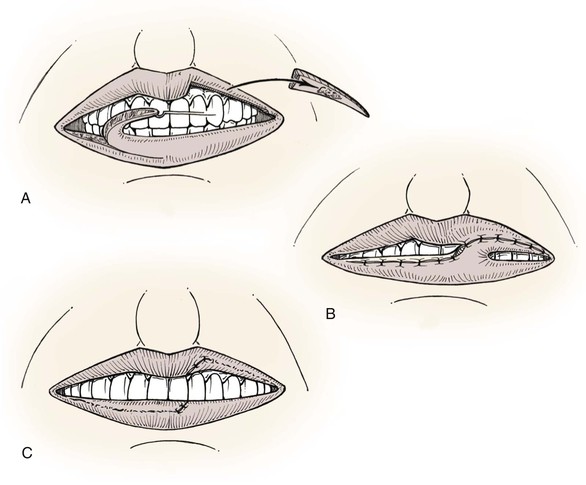
FIGURE 19-7 A, B, Interpolated cross-lip vermilion flap used to reconstruct vermilion defect of upper lip. Donor site repaired by advancing labial mucosa. C, Division of pedicle and flap inset.
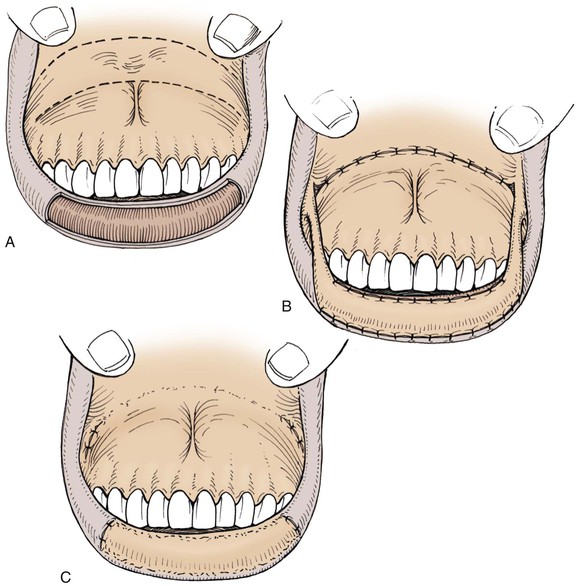
FIGURE 19-8 A, Large defect of lower lip vermilion. Broken lines indicate incisions to create interpolated bipedicle labial mucosal flap. B, Flap transferred to lower lip. Donor site repaired by labial mucosal advancement. C, Pedicles divided and flap inset.



FIGURE 19-9 A, Loss of vermilion of right lateral aesthetic unit of upper lip. B, Unipedicle interpolated cross-lip vermilion flap transferred from lower lip to upper lip. Pedicle must be adequate to accommodate repeated motion of lip during first stage. C, After vermilion cross-lip flap inset to restore vermilion and full-thickness skin graft to replace missing skin of lip.
An alternative design of a cross-lip mucosal flap that does not require an axial pattern vascular supply is a broad flap pedicled on the free margin of the donor lip that can be separated after 16 days.7 Use of this flap causes greater restriction of mouth opening while the pedicle is in place.
Tongue Flaps
Portions of the mucosal surface of the anterior tongue may be transferred to the lip to repair a vermilion defect. A mucosal flap in the form of an interpolated tongue flap is constructed for this purpose (Fig. 19-10).8,9 Mucosa transferred to the lip from the dorsal surface of the tongue will maintain the many fine filiform papillae that are characteristic of the glossal surface. Use of a tongue flap to restore the vermilion will likely create a red vermilion that can be surprisingly satisfactory. A glossal flap is usually harvested from the ventral surface of the tongue for lower lip repair and from the dorsal surface of the tongue for repair of the upper lip. It is also possible to design a flap from the lateral margin of the tongue. In nearly all cases, the pedicle is created at or near the free margin of the tongue. The leading edge of the flap is sutured to the anterior border of the vermilion defect in the best possible manner, anticipating that there will be considerable pulling with tongue movements. Attachment of the flap to the posterior border of the defect is accomplished at a second stage after division of the pedicle and flap inset. The second stage is usually performed 3 weeks after initial flap transfer. The tongue donor site wound may be closed partially or allowed to granulate while the pedicle of the flap remains attached to the recipient lip. Tongue flaps are awkward and difficult for the patient. For this reason, tongue flaps are not considered a first choice for vermilion reconstruction.
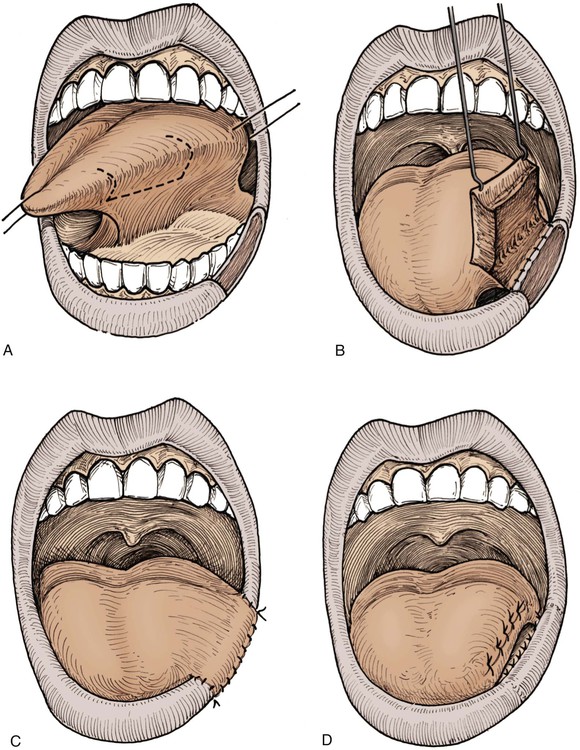
FIGURE 19-10 A, Defect of lower lip vermilion and outline of superiorly based tongue flap. B, Inferior margin of tongue donor site anchored to inner margin of lip defect. C, Tongue flap transferred to vermilion defect. D, Three weeks later, pedicle divided and flap inset, completing reconstruction of vermilion.
Vermilion Advancement Flaps
A full-thickness loss of vermilion and immediate underlying muscle may be a difficult defect to reconstruct. If the defect involves less than one-third of the width of the lip vermilion, it is possible to repair the defect by creating an advancement flap of the remaining vermilion (Fig. 19-11).2,10 A full-thickness incision is made along the anterior vermilion line inferior to the labial artery. The flap includes the vermilion portion of the orbicularis muscle. Flap dissection may require a lengthy incision to allow adequate stretch. A meticulous wound closure is necessary to minimize visible scars in this aesthetically sensitive region.
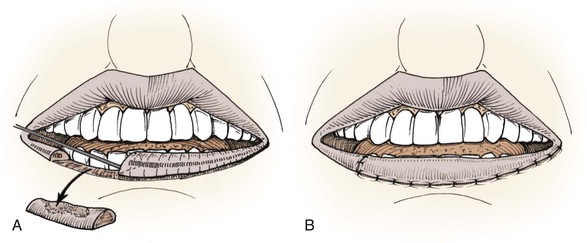
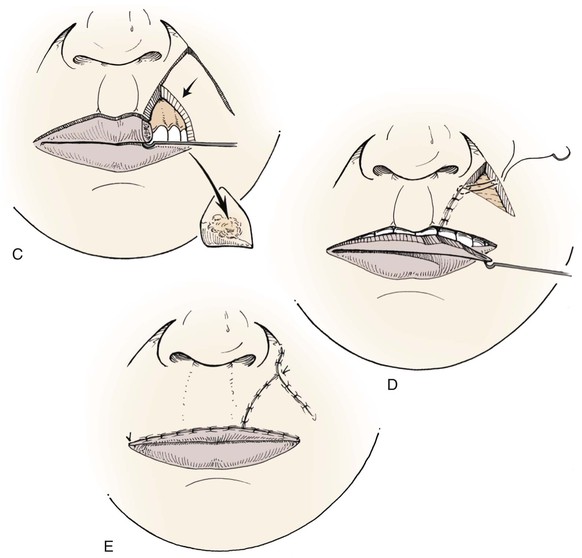
FIGURE 19-11 A, Full-thickness vermilion defect. Full-thickness vermilion advancement flap incised. Bilateral opposing vermilion advancement flaps may also be used. B, Vermilion flap advanced and wound repaired. C, Full-thickness defect of vermilion and adjacent lip. Full-thickness transposition flap and vermilion advancement flap incised. D, Flaps transferred to recipient sites. E, Two flaps in place and wounds repaired.
Cutaneous Reconstruction
The principles of cutaneous lip flap designs are similar to those applicable to other cutaneous surfaces. In reconstruction of the lip, it is preferable to confine tissue movement within the aesthetic region of the lips unless this causes excessive distortion of adjacent structures, such as the melolabial crease. Limitations are imposed on transfer of tissue within the lip complex because of the oral aperture and nasal base. In some cases of reconstruction of the cutaneous lip, it is necessary to include skin from the adjacent cheek or chin. Designing local flaps compatible with relaxed skin tension lines and borders of facial aesthetic regions can provide maximum aesthetic results.
Fusiform Repair
The preferred method for dealing with most cutaneous tumors of the lip remains fusiform excision and primary wound repair. When possible, the fusiform excision is oriented with its long axis parallel to relaxed skin tension lines of that region of the lip. From an aesthetic viewpoint, it is preferable that fusiform excisions be confined within the boundaries of the lip, avoiding extension beyond the melolabial or mental crease lines. An M-plasty at the end of the excision line may be useful in avoiding the need to extend an incision beyond the aesthetic borders of the lips or into the vermilion (Fig. 19-12). This will require closure of two small and slightly diverging incision lines near the involved end. M-plasty may also reduce tissue redundancies, particularly near the free margin of the lip.


Intralabial and Perilabial Flaps
Chin and Submandibular Transposition Flaps
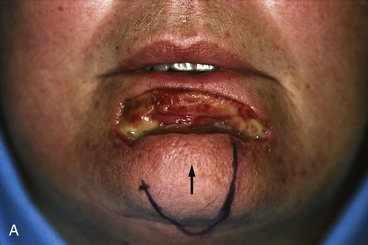
Cutaneous transposition flaps may be transferred to the lips from the chin, submandibular area, or medial cheek. Flaps of the chin may be designed as a single or bilobe flap and may recruit skin from the submental region (Fig. 19-13). The chin is a distinct facial aesthetic region and a highly visible facial feature. Careful planning is important in designing a flap in this region, anticipating exactly what changes will occur in the appearance of the chin after flap transfer. Secondary procedures may be required to restore normal contours, particularly in the region of the mental crease.


Labial Rotation and Advancement Flaps
Labial cutaneous rotation and advancement flaps are used to repair skin defects of either lip. Flaps are designed to move skin medially from the area immediately lateral to the defect. Transfer of such flaps often involves moving skin around the oral commissure in a manner that employs variable degrees of rotation and advancement. The nature of the tissue movement is dependent on the exact location, size, and shape of the defect. Defects located laterally require flaps that are transferred to the recipient site with greater pivotal movement (Fig. 19-14). Defects located medially require flaps that are transferred primarily by advancement. For laterally located upper lip skin defects, rotation flaps are designed so that the lateral border of the flap is in or parallel to the melolabial crease. Flaps may extend inferiorly below the level of the oral commissure on the involved side (Fig. 19-15). Because the distance between the melolabial crease and vermilion diminishes near the oral commissure, the peripheral border of the flap is extended lateral to the crease into the cheek as necessary to achieve adequate flap width. Careful flap design is required to ensure that the width of the flap provides adequate vertical height to the reconstructed lip.
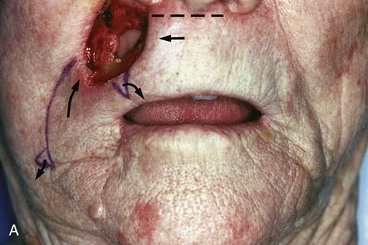


FIGURE 19-14 A, Full-thickness upper lip defect. Mucosal defect closed primarily. Majority of orbicularis muscle sphincter remained intact. Large rotation flap designed for repair. Broken line indicates additional small advancement flap from central region of lip used to lessen wound closure tension. Small curved arrows indicate excision of standing cutaneous deformity of upper lip and an equalizing Burow triangle of cheek skin. B, Wound repaired. Note elevation of right oral commissure resulting from transfer of lateral lip flap. C, One month postoperatively. Commissure in favorable position because of pull of facial musculature. Melolabial crease on surgical side is more lateral in position compared with its counterpart. Appearance of lip is relatively natural.



FIGURE 19-15 A, A 3 × 3-cm cutaneous defect of upper lip. Curved broken line indicates incision to create rotation advancement flap used to reconstruct defect. Triangle in alar-facial sulcus indicates excision of an equalizing Burow triangle of skin. B, Flap in place. C, One year postoperatively. No revision surgery performed. Care is taken with this surgical approach to minimize distortion of philtrum and nasal base.
Dissection of labial rotation and advancement flaps is in the subcutaneous tissue plane superficial to the level of the orbicularis and facial muscles. For rotation flaps, a longer wound border is expected in the cheek lateral to the flap. This disparity in wound length can usually be accommodated by equally dividing the skin redundancy during wound closure. If necessary, a small equalizing Burow triangle of skin is excised from the cheek opposite the most inferior portion of the flap or in the alar-facial sulcus.11
Cutaneous lip rotation flaps are most frequently employed to repair defects involving the more lateral portion of lip skin (see Fig. 19-14). In contrast, advancement flaps are most commonly used to repair centrally located cutaneous defects. As the flap is advanced medially, its base often overlaps the oral commissure. This redundancy of skin at the commissure may require excision. In more extreme cases, the oral commissure may be pulled superiorly or inferiorly with medial advancement of the flap. This may be self-correcting as the natural pulling of the lip musculature causes a corrective adjustment over time (see Figs. 19-14 and 19-15).
Melolabial Flaps
Melolabial cutaneous transposition flaps may be designed with a pedicle that is either superiorly or inferiorly based. A flap with a superiorly based pedicle is commonly used to reconstruct defects of the central upper lip. A flap with an inferiorly based pedicle is often used to reconstruct defects involving more lateral portions of the upper or lower lip. Use of melolabial flaps to repair the lips incurs some degree of flattening of the melolabial folds. Flaps with a superiorly based pedicle produce the greatest degree of distortion of the melolabial fold as they extend across the most defined and visible portion of the fold. A second surgical stage involving revision of the pedicle to align scars parallel to the melolabial crease is frequently indicated in cases in which a melolabial transposition flap is used to reconstruct the upper lip.
Distortion of the melolabial fold and crease, alteration in the orientation of facial hair growth pattern, and tendency toward development of trap-door deformity are reasons that melolabial cutaneous transposition flaps are not frequently used to repair skin defects of the lips. Cutaneous defects in the central portion of the lip are often best reconstructed with bilateral advancement flaps. Larger (≥2 cm) central defects usually are converted to full-thickness defects and closed primarily (Fig. 19-16). Similar to centrally located defects, small laterally located cutaneous defects of the lip can be closed with bilateral advancement flaps, often in the form of an A-T plasty (Fig. 19-17). Larger (≥2 cm) laterally located cutaneous defects of the upper lip are effectively reconstructed with V-Y subcutaneous tissue pedicled melolabial advancement island flaps (see Chapter 12) (Fig. 19-18). The flap is freed from its orbicularis muscle attachments near the commissure and is based solely on the abundant subcutaneous fat located just lateral to the commissure. This is only when the flap is sufficiently large to necessitate the incorporation of skin of the melolabial fold into the flap.

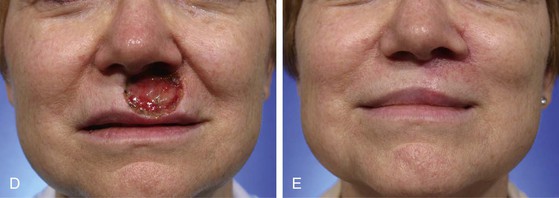
FIGURE 19-16 A, A 2 × 2-cm skin defect of upper lip. B, C, Defect converted to full thickness, sparing most of the exposed muscle, and wound closed primarily. D, E, Preoperative and 1-year postoperative views. No revision surgery performed. (Courtesy of Shan R. Baker, MD.)
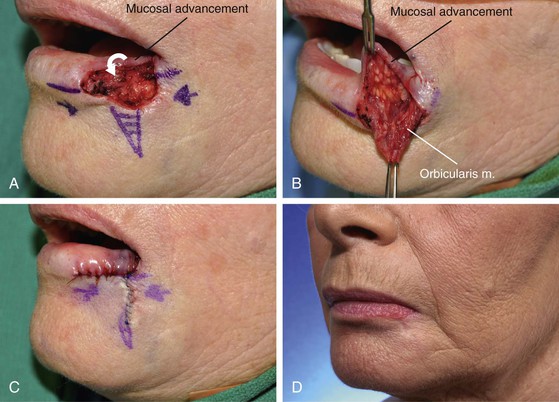
FIGURE 19-17 A-C, A 1 × 1.5-cm skin and vermilion defect. Bilateral advancement flaps (A-T plasty) designed to repair cutaneous component of defect. Mucosa advanced to reconstruct vermilion (arrow). D, Postoperative result at 10 months. No revision surgery performed. (Courtesy of Shan R. Baker, MD.)
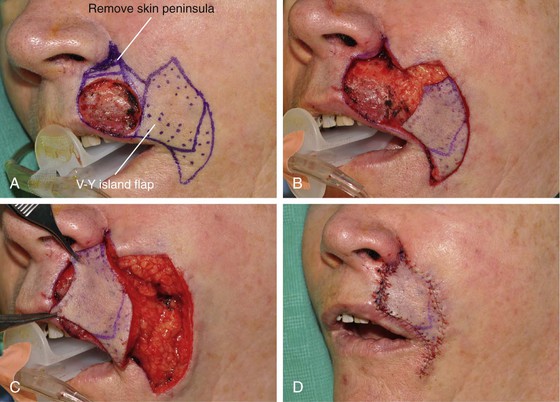

FIGURE 19-18 A, A 2 × 2.1-cm skin and vermilion defect of lip. V-Y subcutaneous tissue pedicled lip advancement island flap designed for repair. Flap designed to recruit medial cheek skin. Non-stippled area represents subcutaneous vascular pedicle on which flap is based. Peninsula of skin in alar-facial sulcus replaced with flap to maximize scar camouflage. B, In situ flap incised. C, D, Flap advanced to recipient site. E-G, Preoperative and 5-month postoperative views. No revision surgery performed. (Courtesy of Shan R. Baker, MD.)
For sizable (2-3 cm) lip skin defects adjacent to the inferior border of the ala, it may be beneficial to excise the small peninsula of skin between the ala and melolabial fold in the process of enlarging the defect so that the defect extends to an aesthetic boundary.8 The peninsula is then reconstructed by appropriately designing the island flap so that the superior portion of the flap replaces the peninsula (Figs. 19-18 and 19-19). This technique provides the best camouflage because the superior border of the flap is positioned within the aesthetic boundaries of the alar-facial sulcus and melolabial crease. When this peninsula is not replaced, the flap must cross the base of the peninsula and may mar an otherwise excellent result.
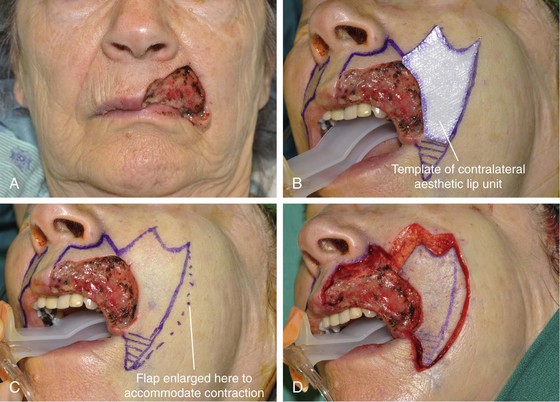

FIGURE 19-19 A, A 3.8 × 2.8-cm defect of skin, vermilion, and muscle of lip. B, Excision of remaining skin of lateral aesthetic unit planned. Template of contralateral aesthetic lip unit used to design V-Y subcutaneous tissue pedicled melolabial rotation advancement island flap. C, Flap width enlarged 1 cm to accommodate scar contracture and subsequent diminution of vertical height of reconstructed lip. D-F, Flap transferred to recipient site. Labial mucosa advanced outward to reconstruct vermilion. G, H, Eight months after reconstruction and 2 months after contouring of flap and Z-plasty scar revision. (Courtesy of Shan R. Baker, MD.)
The major advantage of subcutaneous tissue pedicled melolabial advancement flaps used to repair sizable cutaneous defects of the upper lip is that there is no need to resect standing cutaneous deformities because these do not develop with this flap. For this reason, they are particularly advantageous compared with transposition and cutaneous pedicled advancement flaps, which often have sizable deformities that must be resected and discarded. There is no wasted skin with the island flap. Another important advantage of the island flap is that there is considerably less dead space beneath the flap as well as beneath skin surrounding the donor defect compared with use of cutaneous pedicled flaps. Less dead space means less space available for collection of blood and serum. Therefore, there is less risk for development of a hematoma compared with use of other types of flaps.
Full-Thickness Reconstructions
Primary Repair
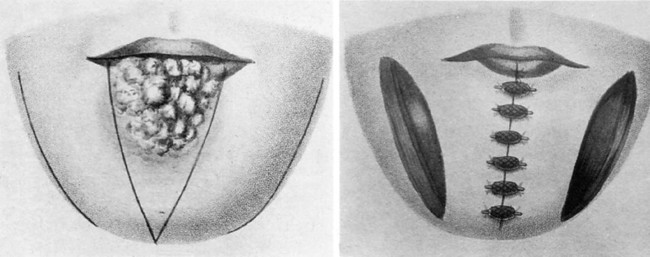
Primary repair of either lip provides satisfactory results for full-thickness defects of as much as one-third the width of the lip. Wedge or V-shaped full-thickness lip excision and primary wound closure have long been the most common method of treatment of most malignant neoplasms of the lip (see Fig. 19-20). Closure of the V-shaped defect is oriented parallel to relaxed skin tension lines of the lip. In the central portion of the lip, the V-shaped excision is oriented vertically, with equal length given to the two borders of the V (Fig. 19-20). In more lateral regions of the lip, the V is skewed to produce a more angulated wound closure line matching the natural relaxed skin tension lines of the lateral lip (Fig. 19-21).


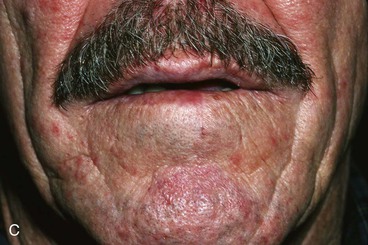
FIGURE 19-20 A, Lip marked for V-shaped full-thickness excision of lip malignant neoplasm. B, Immediately after excision and multilayer wound repair. C, Postoperative result at 6 months. Scar is flat, and notching of vermilion border is not observed.

FIGURE 19-21 Lip marked for V-shaped excision. V is skewed to accommodate slanted relaxed skin tension lines in lateral region of lip.
Optimal primary repair of full-thickness lip defects requires approximation of at least four tissue layers: mucosa, muscle, subcutaneous tissue including deep dermis, and epithelium of the skin. The tendency toward development of a retracted and depressed lip scar is appreciably reduced when the wound is repaired with accurate approximation of the lip muscle. Precise approximation of the subcutaneous tissue layer is accomplished with sutures that are adjacent to or include the deep portion of the reticular dermis. The epithelium of the skin is closed in a manner that ensures a slight eversion of the skin edges. Attention to detail throughout wound closure will achieve an optimal scar that is narrow and flush with adjacent lip tissue.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


