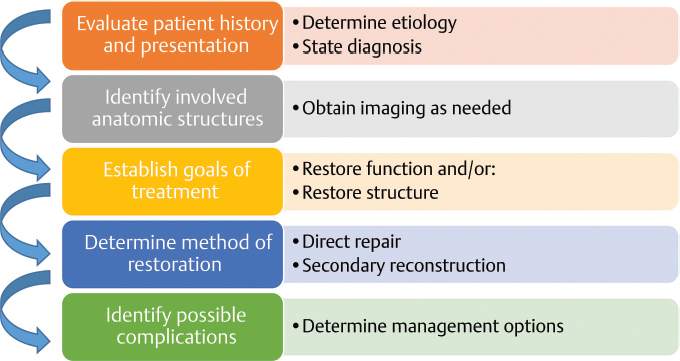
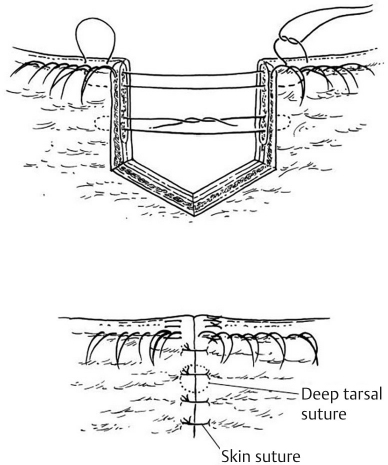
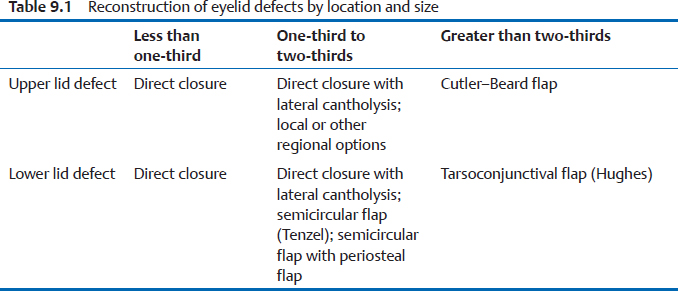
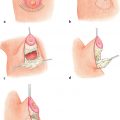
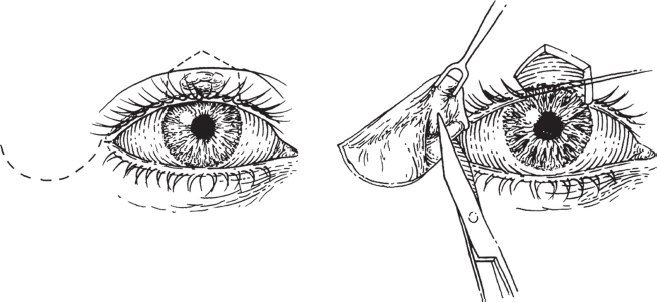
9 Reconstruction of the Facial Defect Abstract This chapter will review reconstructive options for reconstruction of the eyelids, ears, nose, cheek, and mouth. It will be linked to drawing/photographs in an appendix for reader practice of flap design and marking. The reader will evaluate the defect and prioritize flaps for the reconstruction of eyelid, ear, nose, cheek, and lip defects. Keywords: facial defect, eyelids reconstruction, ear reconstruction, nose reconstruction, cheek reconstruction, lip reconstruction Six Key Points • Characterize all facial defects by size and involved lamellae. • Reconstruction will be based on size and involved lamellae by algorithm. • Always await final pathology prior to reconstruction. • If final pathology is not known, many defects can be temporized with skin grafts. • The majority of defects can be managed with local or regional flaps. • Know at least two options for any given defect. A 47-year-old woman comes for discussion of eyelid reconstruction after excision of a resection of a basal cell carcinoma. 1. What are your reconstructive goals? Reconstructive goals in the eyelid are threefold: to restore the height and length components of the eyelid, to restore the function of globe protection, and to avoid complications, such as tethering, that reverse or prevent accomplishment of structural and mechanical restoration. 2. How do you analyze the defect? Analysis is systematic, and considers the etiology, which includes assessment of zone of injury (ZOI), the anatomic defect, and the available tissues for reconstruction. The etiology includes senescent changes, traumatic defects both controlled (such as surgical defects for tumor extirpation) and traumatic. In addition, there are both acute and chronic ZOI considerations. An acute ZOI consideration is a traction injury, which may damage the canaliculi. A chronic ZOI consideration is previous radiation or periorbital surgery, or senescent changes, which may affect reconstructive options (Fig. 9.1). The anatomic defect must be assessed in both the medial–lateral extent and the superficial to deep extent, which includes the bilamellae, the lacrimal drainage system, and the ligamentous support of the eyelid (“tarsoligamentous sling”).1 The anterior lamella of the upper and lower lids contains the skin and orbicularis muscle. The middle lamella contains the orbital septum, fat, and eyelid retractors. The posterior lamella contains the tarsal plate and the nonkeratinized conjunctiva. 3. How might senescent changes or previous surgery affect reconstructive options? In general, the percentage of the eyelid that is affected is a major determinant of the type of reconstruction performed. Scarred or irradiated tissue may have decreased laxity, which may mean that only smaller defects can be reconstructed with certain methods. Similarly, increased laxity may mean that larger defects can be reconstructed. 4. There is a partial-thickness defect of the lid. How do you repair it? The approach to reconstruction needs to include the anterior lamella and the posterior lamella. The anterior lamella can be reconstructed with a skin graft, assuming there is an adequate bed. Full-thickness skin graft donor sites can be excess eyelid skin, preauricular or posterior auricular skin, or supraclavicular skin. 5. The defect is a full-thickness defect that is 20% of the lower lid. What do you do? For full-thickness defects of the lower or upper lid that are less than 25% of the lid, the lid can be directly closed. The edges can be cut into a pentagonal configuration (Fig. 9.2) and the lid edge is closed with 6–0 sutures that come out through the gray line, the tarsal plate is repaired with 6–0 chromic, and the skin is closed with 5–0 fast gut suture. 6. As you attempt to close the lid, it doesn’t quite reach without tension. What do you do? A lateral canthotomy can be performed if the tissues appear to have tension, and are often required with defects 20 to 30% of the lid length. The canthotomy site is closed with suture to create a sharp canthal angle, and if a canthopexy can be performed, it is. 7. The lateral eyelid appears loose. What do you do? A canthopexy can be performed. 8. The defect is 50% of the upper lid. What do you do? A Tenzel semicircular flap. 9. Draw it. The drawing is shown in Fig. 9.3. Fig. 9.2 Pentagonal configuration of lower lid cuts for a closure. (From Chen WP. Oculoplastic Surgery: The Essentials. New York, NY: Thieme Medical Publishers; 2001.) Fig. 9.3 Tenzel’s semicircular flap. (From Chen WP. Oculoplastic Surgery: The Essentials. New York, NY: Thieme Medical Publishers; 2001.) 10. The patient has a prior canthotomy. Can you still perform the Tenzel flap? No. The Tenzel skin–muscle flap requires an intact lateral canthal tendon. 11. The defect is 75% of the upper lid. What do you do? A lid-sharing flap such as a Cutler–Beard flap is appropriate. 12. Describe the flap and draw it. The Cutler–Beard flap can be used for rectangular defects and takes skin, orbicularis muscle, and conjunctive from the lower lid. A cartilage graft to replace the tarsal defect can be sandwiched between the layers of the graft and sutured into place (Fig. 9.4). 13. The defect is 75% of the lower lid. What do you do? A Hughes tarsoconjunctival flap can reconstruct defects greater than two-thirds of the lower lid. 14. Describe the flap and draw it. The Hughes tarsoconjunctival flap is designed on the conjunctival surface of the upper lid. A rectangle is created on the conjunctival surface of the upper lid, at least 3 mm cranial to the lid margin. The dissection can include Muller’s muscle or not, and the dissection proceeds from caudal to cranial including the tarsal plate. Once the flap is freed, it is advanced and sutured into the conjunctiva and lower lid retractors. This reconstruction addresses the posterior lamellae; the anterior lamella needs to be covered with either a skin graft or an advancement flap (Fig. 9.5). 15. When do you divide the flap? The flap is divided between 4 and 6 weeks. It is divided slightly more cranial than the margin to allow for retraction. Fig. 9.4 Cutler–Beard flap. (From Sherris DA, Larrabee WF. Principles of Facial Reconstruction: A Subunite Appraoch to Cutaneous Repair. New York, NY: Thieme Medical Publishers; 2009.) 16. After you divide the flap, you notice elevation of the upper lid. What do you do? Under anesthesia, you can evert the upper eyelid and divide bands of scar. 17. The lower lid is too high. What do you do? Direct excision of the lower lid can reduce the height. The posterior lamella can be reconstructed with a tarsoconjunctival graft. 18. Describe how you take the tarsoconjunctival graft. The tarsoconjunctival graft is taken from the upper lid. At least 4 mm of the caudal border of the tarsus is left in situ to maintain integrity of the upper lid tarsus, and 2 mm of conjunctiva is harvested on the superior border—this is used to reconstruct the lid margin. The donor site heals by secondary intention. 19. That fails. What do you do? A hard palate mucoperiosteal graft is a secondary option for posterior lamella reconstruction. 20. Why wasn’t it your first choice? The donor site morbidity is more significant with a hard palate graft than with a tarsoconjunctival graft, and there is a potential for corneal irritation from the epithelium of a hard palate graft. Fig. 9.5 Hughes tarsoconjunctival flap. (From Janis JE. Essentials of Plastic Surgery. 2nd ed. New York, NY: Thieme Medical Publishers; 2014.) 21. You can’t harvest hard palate mucoperiosteum. What other graft options do you have? Nasal chondromucosal and auricular cartilage. 22. What other options are there for reconstruction? A tarsomarginal graft can be used which is a 7- to 8-mm, wedge-shaped composite graft of the tarsus, conjunctiva, and lid margin. Once this is placed, the anterior lamella is covered with a myocutaneous flap. 23. She comes back 1 year later and complains that she has no eyelashes. What do you tell her? Part of the initial discussion is that eyelashes may not survive on a tarsomarginal graft. After Mohs resection, a patient has a defect that is 20% of the upper lid. 1. What do you do? A 20% defect of the upper lid can be repaired primarily. If there is significant laxity, as in the elderly, larger defects can be repaired with direct closure, and cantholysis can increase the percentage defect to 50%. 2. The defect of the upper lid is 50 to 60%. What do you do? The Tenzel semicircular flap is a great option for defects ranging from 40 to 60% of both upper and lower lids (Table 9.1). 1. Describe your approach to the ear defect. The ear is first assessed regarding the structures of the ear that are involved. This principle does not apply to If there is pre-existing pathology, such as effacement of the antihelical fold, prominence of the concha—both of which may lead to a prominent ear—this is assessed. Asymmetry of the ear is also assessed. Finally, the amount of defect is estimated as a percentage of the ear. The helical rim, sulcus, and antihelical fold are evaluated as subunits of the ear. 2. A patient presents after resection of a basal cell carcinoma of the helical rim. The defect measures 1.5 cm. What do you do? A helical rim defect that measures 2 cm or less can be closed with an Antia–Buch flap.
Questions
Eyelid Reconstruction
Case 1
Upper Eyelid Reconstruction
Case 2
Ear Reconstruction
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine