Reconstruction of The Cervical Esophagus by Visceral Interposition
C. E. SILVER
R. J. BRAUER
Various segments of abdominal viscera may be transposed or freely transplanted to replace portions of esophagus after resection or stenosis. The main advantage of these procedures, compared to reconstructions using skin (see Chapter 215), is that considerably longer segments of esophagus can be replaced. Visceral interpositions often can be performed in a single stage, thus permitting rapid rehabilitation of the esophagectomized patient; however, the magnitude of surgical trauma is generally greater than with skin reconstructions, and potentially disastrous complications may occur in association with necrosis or anastomotic failure. Thus, a greater degree of risk is assumed with these procedures than with reconstructions using skin to replace esophagus.
INDICATIONS
Reversed Gastric Tube
An antiperistaltic gastric tube (1) has been found to have several advantages over isoperistaltic tubes (2, 3, 4), including greater length, simplicity, and versatility, and has been more widely employed (Fig. 224.1).
Esophagocoloplasty
The colon generally provides a slightly shorter conduit than can be created by a reversed gastric tube and is more difficult to transfer subcutaneously. Thus, we tend to use colon more often in patients in whom substernal transfer is feasible or in whom anastomosis to the lower cervical esophagus is required (5) (Fig. 224.2).
Despite arguments advanced by advocates of either esophagocoloplasty or gastric tube esophagoplasty, the choice of procedure depends more on the experience and familiarity of the individual surgeon with either method than on any marked inherent advantage of one over the other.
Gastric Transposition (Gastric Pull-Up)
The gastric pull-up operation offers several advantages over other visceral interpositional procedures (6, 7, 8, 9, 10, 11). The blood supply of the transposed stomach is superior to that of colon and reversed gastric tube. The procedure is performed in one stage, and the only anastomosis is extraabdominal, which lessens the chance of peritonitis or mediastinitis. The pharyngogastric anastomosis is particularly resistant to strictures and dehiscence. Elimination of the thoracotomy markedly lessens the morbidity and mortality of the procedure. When employed in properly selected patients, the gastric transposition operation comes close to being the ideal method for pharyngoesophageal reconstruction (see Chapter 215). There are, however, limitations.
The gastric transposition operation for resection and reconstruction of cervical esophageal carcinoma combines the advantages of two concepts. The scope of resection is increased by including extrathoracic extraction of the entire esophagus with the resection. Reconstruction is then accomplished by pulling the entire stomach through the posterior mediastinal bed of the resected esophagus to the level of the pharynx, to which it is anastomosed. The procedure is performed in a single stage and is technically simpler than other methods of visceral interposition. The well-vascularized stomach is a most reliable esophageal substitute (Fig. 224.3).
ANATOMY
Reversed Gastric Tube
The reversed gastric tube is pedicled at the fundic end of the stomach and is based on the left gastroepiploic vessels. With splenectomy and mobilization of the tail of the pancreas, a sufficiently long conduit can be developed to easily reach the level of the oropharynx (Fig. 224.1).
Esophagocoloplasty
Both right and left colon can be used for esophageal replacement. In theory, the right colon has the advantage of assuming an isoperistaltic orientation after interposition; however, a great length of the left colon can be pedicled on the middle colic vessels, and angiographic studies (12) confirmed that the
marginal artery of the colon is more consistent on the left side. Although the left colon assumes an antiperistaltic orientation when interposed, this has not proven functionally significant (Fig. 224.2).
marginal artery of the colon is more consistent on the left side. Although the left colon assumes an antiperistaltic orientation when interposed, this has not proven functionally significant (Fig. 224.2).
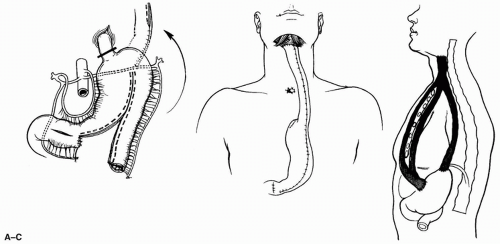 FIGURE 224.1 Reverse gastric tube esophagoplasty. A: Pedicled tube from greater curvature. B: Final position of tube with anastomoses to pharynx. C: Alternate routes for tubed transfer to neck (subcutaneous, substernal, and posterior mediastinal). (From Silver, ref. 13, with permission.) |
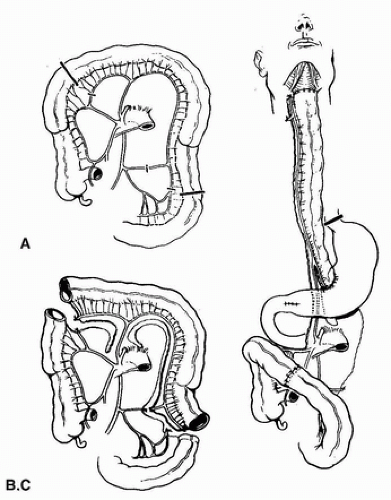 FIGURE 224.2 Esophagocoloplasty (left colon). A: Blood supply of colon—outline of transposed segment. B: Colon mobilized. C: Final position of interposed colon. (From Silver, ref. 13, with permission.)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





