Reconstruction of Contractures: Z-Plasty, Skin Grafting, and Flaps
Xiangxia Liu
DEFINITION
Scar contracture is the result of tightening of the skin during and after the wound healing process.
The continuous and progressive contraction of the scar will cause the impairment of appearance and significant dysfunction of the affected area.
In the lower extremities, especially around the knee and ankle joint, the contracture scar can cause significant restriction in movement and, therefore, should be treated as soon as possible.
There are many surgical interventions to treat scar contracture, including Z-plasty technique for mild scar contracture, skin grafting for a larger area of skin defects after the releasing of the contraction, and a skin flap, especially around the knee and ankle joint area or when there are any bone, tendon, nerve, and blood vessel exposure.
ANATOMY
The scar contractures in the lower extremities usually only affect the superficial fascia layer. Sometimes there will be exposed bone, tendons, nerves, and vessels after scar resection or revision.
Lateral femoral circumflex artery (LFCA) arises from the deep femoral artery; it goes deep to the rectus femoris muscle and divides into three branches: the ascending, transverse, and descending branch. The Anterolateral thigh flap (ALT) is designed base on the perforator of the descending branch of LFCA (FIG 1A).
Pedicled reverse-flow ALT flap is a useful tool to repair the defects around the knee joint. The descending branch of LFCA will communicate with the arteries around the knee joint, which perfuses the pedicled reverse-flow ALT flap (FIG 1B).
PATIENT HISTORY AND PHYSICAL FINDINGS
Patient history and physical examinations will help us to determine whether a simple Z-plasty can release the contracture or skin grafting or a flap is needed (FIG 2).
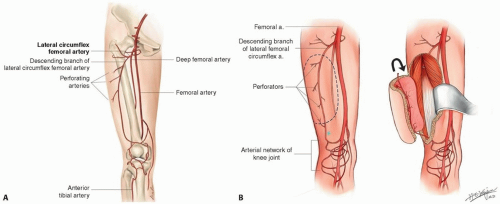 FIG 1 • A. Arising from the produnda femoral trunk, the lateral circumflex femoral artery (LCFA) gives three branches: ascending, transverse, and descending branch. The descending branch of LCFA travels deep with the space between the rectus femoris muscle and the vastus lateralis muscle. As traveling distally, it distributes the perforators, in most cases musculocutaneous perforators to the flap. B. The distal communicating artery between the descending branch of LFCA and the lateral superior geniculate artery is the anatomic basis for the reversed ALT flap. |
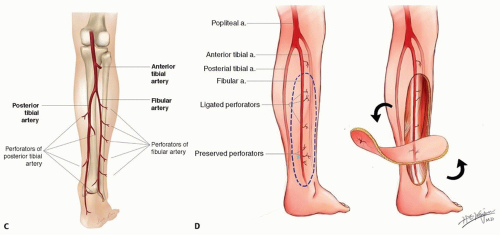 FIG 1 (Continued) • C. Through its course in the leg, the posterior tibial artery usually gives two to four major septocutaneous perforators; these perforators arise from between the soleus and the flexor digitorum longus muscle or between the flexor digitorum longus muscle and the medial aspect of tibial bone. The distance between the lowest perforator and the medial malleolus ranges from 3.5 to 8.2 cm.1 D. The perforators of peroneal/fibular artery arise from between the soleus and the peroneus longus/brevis muscle. They are usually located within 2 cm from posterior border of fibular bone and are closer to the fibular bone proximally than distally. |
IMAGING
Preoperative radiography can help to distinguish simple and complex scar contracture, especially if an underlying skeletal abnormality is suspected.
CT and MRI scanning play an important role in the evaluation of skin cancer.
An MRI can well identify the relationship among the tumor, calcaneus bone, and Achilles tendon in the case of Marjolin ulcer, an aggressive squamous cell carcinoma presenting in an area of chronic inflammatory scar tissue (FIG 3).
SURGICAL MANAGEMENT
Indications
Z-plasty is designed to elongate a less contracted linear scar or to break a scar tension line.
Skin grafting is an option when the primary closure is impossible and there is a lack of adjacent tissue for coverage.
Flap should be applied when there is an exposure of the bone, nerve, blood vessel, and other tissues, which are unsuitable for skin graft.
Preoperative Planning
Prepare the donor site for skin grafting.
Use Doppler ultrasonography to confirm the perforator before the operation.
Pathological study of the chronic ulcer in the scar area before the surgery is important.
Positioning
The patient is placed supine on the operating room table with the entire lower extremity prepared into the field.
The ipsilateral or contralateral thigh is prepared into the field in the event that a split-thickness skin graft is needed.
The scalp is another option for harvesting thin split-thickness skin grafts if the patients do not want to leave a visible scar on the donor site.
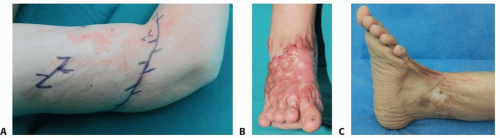
FIG 2 • A. For a superficial nonhypertrophic scar on right arm with minimal contracture, the simple technique of Z-plasty will release the contracture scar and break the tension line. B. For this patient, skin grafting is needed to replace the unwanted hypertrophic scar on the dorsum of the right foot and to release the dorsal contracture of the second, third, and fourth toes. C. Both the Z-plasty and skin grafting are needed to fully release the contracture bands of the left ankle and foot.
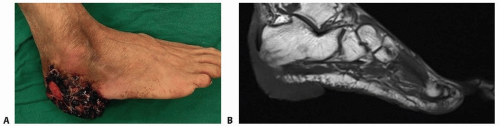
FIG 3 • A. Cauliflowerlike tumor on the right heel. B. MRI shows the tumor has a close relationship with the calcaneus bone and the Achilles tendon. A flap would be needed to cover this defect after tumor resection because there will be an exposure of both the bone and tendon.
The groin is prepared in the event that a full-thickness skin graft is needed.
A prone position will be helpful when the procedure is related to the posterior aspect of lower extremity.
A lateral decubitus position will facilitate the exploration of the perforator of peroneal artery.
Approach
Make the incision on the medial margin of ALT flap first as this will facilitate the exploration of perforators in the medial thigh in case that there is no perforator available in the lateral side.
TECHNIQUES
▪ Z-Plasty
Draw the center line on the part of the scar with the most contracture.
Make a paired and paralleled limb line on each side of the center line (TECH FIG 1A).
Try to set the angle around 60 degrees between the center line and limb lines.
Cut the skin along the designed lines.
Release the subcutaneous bands.
Elevate the flap superficial to the deep fascia (TECH FIG 1B).
Transpose the paired skin flaps (TECH FIG 1C).
Trim the dog ears and overly abundant subcutaneous tissues.
Place several sutures in dermal layer of the key areas.
Close the wound accordingly.
 TECH FIG 1 • A. Multiple Z-plasties marked on a contracture band. B. The flap is elevated superficial to the deep fascia. C. The paired Z-plasty flaps are transposed initially. |
▪ Skin Grafting Preparation of the Recipient Site
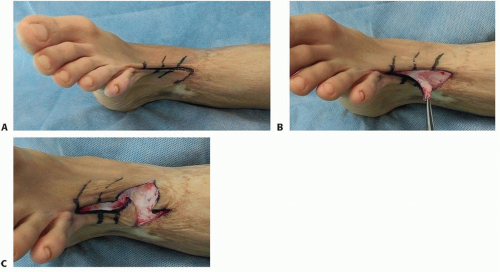
Release the contracture bands of the scar (TECH FIG 2A).
Make multiple zigzag incisions along the cutting edge of the wound to lessen the tension of the scar (TECH FIG 2B,C).
Remove the scar tissues in the wound.
Control bleeding with bipolar electrocautery.
Make a template of the defect.
Harvesting the Skin Grafts
Use the tumescent fluid to flatten the surface of donor site and reduce bleeding.
Use a power-driven (TECH FIG 3A) or freehand dermatome to harvest the split-thickness skin grafts from the thigh or scalp.
Choose the width and the thickness of the harvested grafts by adjusting the dermatome (TECH FIG 3B,C).
A simple way to assess the thickness is by passing a no.15 blade between the guard and the blade.
Install and lock a new disposable blade.
Make a 30- to 45-degree angle between the handle and the surface of the skin (TECH FIG 3D).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree