Amputation of the Lower Extremity: Toes, Foot, Ankle
Kedar S. Lavingia
Jason T. Lee
INTRODUCTION
Partial foot amputation (PFA) is a common sequel to advanced vascular disease secondary to diabetes and its complications.1
PFA may also occur due to injury, infection, cancer, or birth defect.
PFA affects approximately 2 per 1000 patients in western countries, making it the most common type of amputation surgery.2
PFA is associated with a significant failure rate and numerous complications including skin breakdown, ulceration, and equinus contracture, which can lead to subsequent and more proximal amputation.
Thoughtful patient selection, early involvement of neuropsychiatry and physical medicine and rehabilitation (PM&R) are fundamental to a successful outcome.
BACKGROUND/CONSIDERATIONS
Forefoot Amputation
Toe disarticulations are quite challenging when dealing with the remaining cartilage of the involved metatarsal head and possible complications of residual osteomyelitis.
Ray amputation, which involves the excision of the toe and part of the metatarsal, provides a more viable option of ensuring an adequate surgical debridement of the septic margins if that is the indication.
Indications may include a wet or dry gangrene of a toe, osteomyelitis of the metatarsal head and/or proximal phalanx, septic arthritis of the metatarsophalangeal joint, and gross infection of the toe.
Suggested inclusion criteria by a variety of authors for this type of amputation may include one or two palpable pedal pulses, ankle brachial index (ABI) ≥ 0.8, and toe brachial index ≥ 0.7.3
In recent studies, absence of pulses, delayed capillary filling, high erythrocyte sedimentation rate, high creatinine, and high neutrophil counts were found to be predictive factors for a poor clinical outcome.4
Indications for transmetatarsal amputation may include wet or dry gangrene involving only the forefoot and/or infection involving the forefoot, whereas the inclusion criteria are the same as those mentioned above required for a ray amputation.
Midfoot Amputation
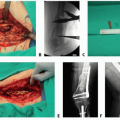
Lisfranc disarticulation is a disarticulation through the tarsometatarsal joint, whereas Chopart disarticulation is a disarticulation through the talonavicular and calcaneocuboid joints leaving only the hindfoot (talus and calcaneum) behind (FIG 1).
These amputations are rarely performed in diabetic foot infections due to high failure rate and the proximity of infected tissue to the heel pad.7
Hindfoot/Ankle Amputation
This category included the amputations such as Syme amputation and has the indications and inclusion criteria as mentioned in the forefoot amputation category (FIG 2).
Syme amputation has been advocated for trauma cases; however, Syme amputation can give good results in patients with diabetic foot infections.8
Syme amputation should be reserved for patients with at least a palpable posterior tibial pulse and an ankle-brachial index of more than 0.5.
SURGICAL MANAGEMENT
Preoperative Planning
All patients undergoing an amputation should be evaluated by both neuropsychiatry and PM&R early.
Prevention and early detection of future disease should be discussed with the patient.
Education on pressure-area pathogenesis is important as part of a strategy to encourage the patient to prevent further problems.Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Tibial Reconstruction
Tibial Reconstruction
 Femoral Bone Debridement
Femoral Bone Debridement
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


