CHAPTER 50 Reconstruction of Acetabular Bone Deficiencies Using the Antiprotrusio Cage
One of the most challenging aspects of acetabular revision is managing bone loss. Bone loss occurs in a variety of locations, and bony defects are of variable size. The goal is to create a stable construct capable of providing long-term stability of an acetabular component.1
Most acetabular defects can be reconstructed with an uncemented hemispherical cup with screws with or without bone graft. Significant acetabular defects may require structural grafts, a bilobed cup, a trabecular metal cup with or without augments, an acetabular protrusio cage, or a cup-cage construct depending on the type of bone loss.2 An unresolved issue in revision total hip arthroplasty (THA) is acetabular reconstruction when extensive bone loss is significant enough to exceed the limits of large hemispherical cups.3
The antiprotrusio cage (APC) provides a large contact area between the implant and remaining pelvic bone, distributes force over a large area, and decreases the likelihood of implant migration.4 It also allows the treatment of large bone defects with morcelized or bulk bone grafts, bridging gaps in native bone and thus protecting bone graft from forces that might contribute to failure.5 The APC provides fixation above and below areas of pelvic discontinuity, thereby allowing simultaneous treatment of the discontinuity and the failed acetabular component.
RELEVANT SURGICAL ANATOMY
Vessels
The most commonly cited mechanism of injury of the femoral artery is by way of the anterior retractor that is placed during the surgical approach.6,7 The surgeon must avoid damage by keeping the retractor close to bone, using a blunt-tipped device, and avoiding strong retraction over the lip of the acetabulum.
CLASSIFICATION OF ACETABULAR BONE DEFECTS
The American Academy of Orthopedic Surgeons classifies acetabular bone deficiencies into the following five categories (Fig. 50-1)8:





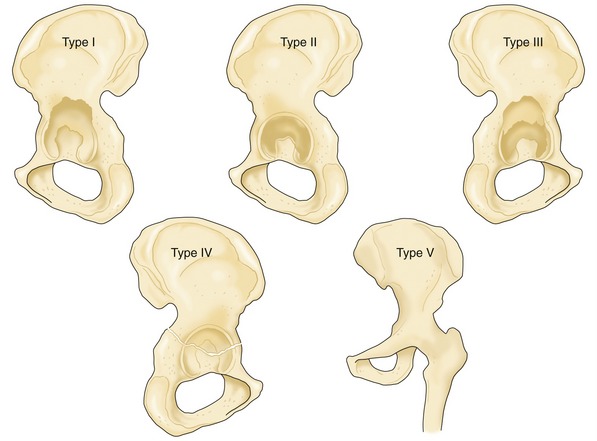
FIGURE 50-1 Acetabular bone defect classification according to the American Academy of Orthopedic Surgeons.
(Redrawn from Macheras GA, Baltas D, Kostakos A, et al: Management of large acetabulum bone defects. Acta Orthop Traumatol Hell 54:1, 2003.)
Berry and colleagues9 subclassified the pelvic discontinuity as type IVa if it was associated only with cavitary bone loss, as type IVb if it was associated with segmental or combined (cavitary and segmental) bone loss, and as type IVc if it was associated with previous irradiation of the pelvis with or without cavitary or segmental bone loss.
Paprosky10 classified acetabular defects as follows (Fig. 50-2):
 Type I—undistorted intact rim, small focal areas of contained osteolysis, Kohler line intact, no structural graft needed
Type I—undistorted intact rim, small focal areas of contained osteolysis, Kohler line intact, no structural graft needed Type II—distorted rim with intact columns, hemispherical acetabulum, <3 cm of superomedial or superolateral migration, small areas of osteolysis at the ischium <7 mm below the obturator line, Kohler line intact; if graft needed, it is needed for augmentation and not for structural purpose
Type II—distorted rim with intact columns, hemispherical acetabulum, <3 cm of superomedial or superolateral migration, small areas of osteolysis at the ischium <7 mm below the obturator line, Kohler line intact; if graft needed, it is needed for augmentation and not for structural purpose Type IIA—superomedial migration, center of acetabulum is <3 cm above the obturator line, Kohler line is intact; if graft needed, it is for augmentation only, not for structural purpose (must have a superior rim capable of containment)
Type IIA—superomedial migration, center of acetabulum is <3 cm above the obturator line, Kohler line is intact; if graft needed, it is for augmentation only, not for structural purpose (must have a superior rim capable of containment)





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


