80
Reconstruction of a Type II Hypoplastic Thumb
Allan E. Peljovich and Peter M. Waters
History and Clinical Presentation
An 11-month-old boy was brought in by his parents for evaluation of his right thumb. At birth, he was noted to have a tethered cord, an imperforate anus, and a small thumb. He had previously undergone surgery on his spinal cord and has had the initial stages of surgery to reconstruct his anus and rectum. He has been referred for possible reconstructive surgery of his hand.
Physical Examination
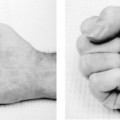
There was mild radial deviation of the carpus of the right arm. The length of the thumb was to the level of the index proximal interphalangeal (PIP) joint. The thumb was adducted, and the patient had a narrowed thenar web space. He had intact flexor pollicis longus (FPL), extensor pollicis longus (EPL), and flexor pollicis brevis (FPB) motion and function. He had noticeable flattening of his thenar eminence, and did not oppose the thumb in play activity. He had complete ulnar collateral ligament instability at the metacarpophalangeal (MP) joint at both 0 and 30 degrees of MP flexion, and passively abducted his thumb through the unstable MP joint, and not through the web space. The carpometacarpal (CMC) joint was stable. He did use the thumb in play and grasp activity, and, in fact, pinched objects between his index and long fingers.
Diagnostic Studies
On radiographs, there appears to be mild ulnar positive variance (Fig. 80–1). The thumb ray is made of a metacarpal and two phalanges, albeit hypoplastic. The carpal ossification is normal for age, with the hamate and capitate ossified.
PEARLS
- Careful assessment of the patient and his or her hand is critical to a good outcome.
- When possible, surgery should be performed before the age of 18 months and ideally at 9 to 12 months of age.
PITFALLS
- Surgeon must be aware of the anatomic variability that can exist, and be flexible in his or her preoperative planning, and intraoperative decision making.

Figure 80–1 Anteroposterior (AP) radiograph of the patient’s hand. There is mild ulnar positive variance, which is suggestive of type I radial dysplasia. The ossified capitate and hamate are consistent with the child’s age; it is too early for ossification of the scaphoid or trapezium. The thumb ray is short.
Differential Diagnosis
Normal variant
Trigger thumb
Severe carpal tunnel syndrome
Any of the variants of hypoplastic thumb per the modified Blauth classification
Diagnosis
Hypoplastic Thumb (Type II) with Probable Type I Radial Dysplasia
Our case illustrates the principles involved in reconstructing most type II and IIIA hypoplastic thumbs. It is important to realize that the spectrum of deficiencies can range from simple shortening of the thumb ray to its complete absence. The choices for treatment include no treatment, surgical reconstruction, amputation, index pollicization, free tissue transfer, and any combination of the former. In 1981, Buck-Gramco expanded upon Blauth’s previous classification system that is helpful in understanding this spectrum and in choosing operative treatment. In 1995, Manske further divided type III hypoplastic thumbs into two variants based on the integrity of the CMC joint. Type IIIA thumbs have an intact and stable CMC joint, whereas type IIIB thumbs do not. The main difference for treatment is that some believe that the lack of a CMC joint precludes any successful attempt at reconstruction, and these thumbs therefore should be amputated. This classification system is illustrated in Table 80–1. Type I hypoplasia is often treated with observation only. Types II and IIIA hypoplastic thumbs are two common variants amenable to surgical reconstruction. Types IIIB and IV are usually treated by amputation and index pollicization. Type V is treated by index pollicization, provided there is a sufficient index finger present. Although our case illustration is that of a patient with type II hypoplasia, the principles involved in assessment and treatment apply to all hypoplastic thumbs.
When examining an infant or child, it is important to take account of the child’s health, as well as to examine the entire extremity. Associated syndromes include VATER (vertebral defects, imperforate anus, tracheoesophageal fistula, and radial and renal dysplasia), Holt-Oram, and Fanconi’s anemia. In 1996, James et al surveyed a large group of patients with hypoplastic thumbs. They found radial dysplasia in 59%, and associated syndromes in 43% of the patients.
| Type | Findings (Additive with Increasing Severity) |
| I | Thumb size diminished. Possible hypoplasia of median innervated thenar intrinsics. |
| II | Deficient/absent median innervated intrinsics. Adduction contracture/web space contracture. Ulnar collateral instability of metacarpophalangeal (MP) joint. |
| III | Deficient/absent ulnar innervated intrinsics. Ulnar and possible radial collateral instability of MP joint. Abnormalities/absence of thenar extrinsics. |
| IIIA | CMC is stable. |
| IIIB | CMC is unstable/proximal phalanx may be absent or deficient. |
| IV | Pouce flottant. No bony support to the present phalanges; only a neurovascular pedicle attaches thumb to hand. Thumb ray carpals deficient/absent. |
| V | Thumb aplasia. |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


