- •
There are lateral and vertical vectors of glabellar frowning.
- •
Glabellar frown vectors are controlled by different muscle groups with unique innervation.
- •
Unique innervations patterns can be identified with the GFX system.
- •
Surgeon uses GFX to produce motor nerve blockade with precise radiofrequency thermal effects.
- •
Percutaneous radiofrequency ablation produces selective clinical effects to improve glabellar frowning.
Introduction
A new minimally invasive procedure is described for the reduction of glabellar frowning. A unique bipolar radiofrequency (RF) device has been developed and used to produce selective denervation of the eyebrow depressor muscles including the corrugator and procerus muscles by a percutaneous minimally invasive route that can be performed in an office based setting. RF energy has been used successfully in cardiac arrhythmias ( ) and facial pain conditions such as trigeminal neuralgia ( , ). The use of RF for the ablation of selected distal branches of the facial nerve for aesthetic benefit is the mechanism of injury procedure. A description of the targeted nerves, patient selection, procedure, and clinical examples will be discussed. As this is both a new technology and procedure, it is important to emphasize that the current techniques and information presented in this chapter represent a work in progress. The findings and clinical results presented here are very encouraging and are being presented to inform the reader about newer approaches in facial aesthetic plastic surgery. Several studies looking at various aspects of this procedure are ongoing at the writing of this chapter.
The presence of glabellar frown lines is a common complaint for which patients seek out treatments from their plastic surgeon. Surveys from the American Society of Plastic Surgery and the American Academy of Facial Plastic Surgery list the use of botulinum toxin A as the most common aesthetic office based treatment of the past 2 years. There has been a heightened public awareness of glabellar frown lines and the use of neurotoxins for their treatment since botox was approved for cosmetic indications to reduce glabellar frowning in 2002. Surgeons have been able to offer alternative treatments to the use of botulinum toxin A with the use of forehead lifts and transpalpebral approaches to resect and/or weaken the corrugator, procerus, and orbicularis muscles groups while in the operating room. These treatments go beyond simple frown reduction and treat lax skin. These surgical procedures have a high level of patient satisfaction when thoroughly performed and when the resulting void is replaced with autologous graft material ( , ). The use of endoscopic approaches has also allowed surgeons to not only perform myectomies and myotomies but also neurotomies providing long-term relaxation of the glabellar complex ( , ).
The concept of percutaneous nerve ablation for branches of the facial nerve was first reported by Herndadez-Zendejas and Guerrero-Santos in 1994. They showed significant reductions in glabellar frowning with long-term follow up to 18 months and a similar study at Stanford showed shorter term results ( ). The current presentation reflects improvements of this original concept by applying a more sophisticated engineered device with a more thorough understanding of facial neuroanatomy. The goal of the GFX procedure is to provide the surgeon with a minimally invasive approach to glabellar frowning without the use of temporary neurotoxins.
The minimally invasive procedure described here uses a radiofrequency needle and generator specifically designed for peripheral motor nerves (GFX Generator, Bioform Medical, San Mateo, CA, USA) ( Figure 3.1 ). The use of this technology to ablate only the efferent pathway of the distal branches of the facial nerve branch as they enter the glabellar musculature can yield a very selective relaxation of the forehead depressor function. This selective efferent nerve ablation provides a non-pharmacologic relaxation of the corrugators, medial orbicularis, depressor supercillii and procerus muscles and thus, produces a relaxation of glabellar frowning. The application of optimized radiofrequency energy has a long history of success in treating various conditions including cardiology applications such as ablation of tachyarrythmias. Previous studies have demonstrated efficacy of application of radiofrequency energy in the human forehead to produce acute and long-term reduction of glabellar furrowing.

Pertinent anatomy
The depressor muscle group is made up of the corrugator supercillii, procerus, orbicularis oculi and depressor supercilli muscles. The corrugator supercillii muscle has both an oblique medial head and lateral transverse head. The lateral transverse head and the lateral orbicularis oculi muscle are innervated by the temporal branch of the facial nerve and are approached through the lateral eyebrow skin as described below. The medial depressors including the medial oblique head of the corrugator, procerus, and depressor supercillii muscle are innervated by the angular nerve.
As the motor nerves to these muscles come from the facial nerve, they run in parallel directions to the facial musculature. The sensory supply to the soft tissue comes from the trigeminal system and emerges from foramina in close proximity to the depressor muscles and are running in a more perpendicular direction to the depressor muscle group to pierce the musculature and then run in a parallel direction to the soft tissues. The differences in the orientation of the sensory and motor nerve supply allow the surgeon to find zones of vulnerability to damage the motor nerves while preserving the sensory nerve supply. The one exception to this, which the surgeon must be aware of, is the deep branch of the supraorbital nerve.
The deep branch of the supraorbital nerve runs in a similar orientation to the lateral frontal motor branch and is separated from it in depth. The motor nerve runs just underneath the muscle body while the sensory nerve is separated by the galea and glide plane as it runs within or just above the periosteum. Whether this nerve emerges from the same foramen as the supraorbital nerve or a separate superolateral foramen, it runs in a parallel direction to the frontal bone and runs within the periosteum or just above it. Because of the orientation of the pathway of this sensory nerve, it can be close to the lateral zone of thermal ablation when the lateral nerve to the corrugator supercillii muscle is being treated. Caution should be exercised to avoid injury to this nerve pathway by preventing the probe tip from pressing down against the periosteum near the lateral border of the corrugator muscle.
The GFX probe is used by the surgeon to locate and ablate both the lateral nerve to the corrugators as well as the angular nerve to the procerus and medial corrugators complex. This is inclusive of the depressor supercilii, oblique head of the corrugators and medial head of the orbicularis in conjunction with the procerus muscle. A brief review of the neuroanatomy is depicted in Figure 3.2 . The course of the frontal branch of the facial nerve has been well described. The distal branches after it crosses the zygomatic arch have four to eight rami which generally form three pathways ( ). The superior pathway goes to the frontalis muscle within the temporoparietal fascia then pierces the under-surface of the frontalis. The most inferior branch innervates the orbicularis oculi muscle and the middle pathway innervates portions of the superolateral orbicularis and the corrugator muscle. The lateral pathway with the nerve to the corrugator is approached in the infrabrow skin just superior and lateral to the lateral canthus. This approach allows the surgeon to move the GFX probe and localize the course of the nerve to the transverse head of the corrugator supercilii muscle.
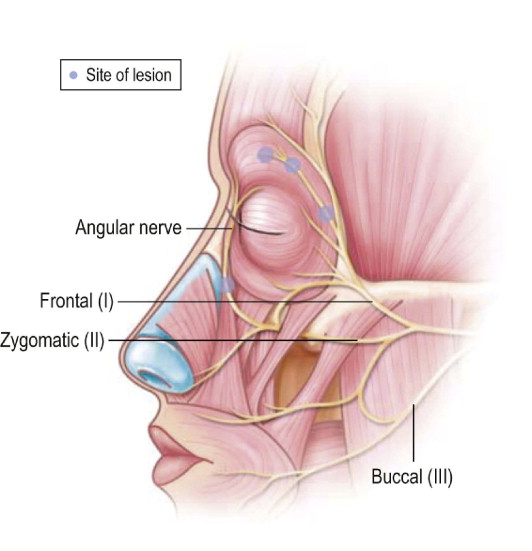
Because the GFX probe has built in stimulation current with the insulated tip, the surgeon is able to confirm location by observing independent muscle contraction of the frontalis, corrugators, and orbicularis depending on the placement of the probe. The stimulation of the lateral branch to the corrugators results in lateral-medial movement of the eyebrow complex. The medial oblique head of the corrugator supercilii muscle, depressor supercilii and the medial head of the orbicularis muscle and the procerus muscle are innervated by the angular nerve ( ). This nerve runs parallel and just posterior to the associated angular artery and vein. This nerve is a branch of the zygomatic nerve and also receives some internuncial communication from the buccal branch. This nerve runs deep to the zygomatic major muscle to emerge in the subcutaneous fat just anterior to the levator anguli oris muscles and adjacent to the levator labii superioris alequae nasi muscle. It is approached with the GFX probe through a skin stab incision just at the superolateral aspect of the nasolabial groove. Stimulation of this nerve results in visible superior-inferior movement of the brow complex.
Operative technique
Evaluation
Patients who are selected for the GFX procedure must undergo a thorough consultation with their surgeon to understand their own aesthetic features, asymmetries, alternative treatments, and risks. It is important to document the patient’s brow complex by discussing the entire forehead and midface region focusing on the horizontal, vertical, and oblique creases in the forehead. In order to assure that the patient’s muscles are being evaluated in their baseline state, neurotoxins should not have been administered for the preceding 3–4 months. Patients are informed about the two sites where the GFX probe will be inserted. One site is just at the outer corner of the orbital rim for the lateral approach and the second is just at the latero-superior aspect of the nasolabial groove for approach to the angular nerve. Still photography without the use of flash is taken with the patient in repose, raising their eyebrows, and in maximum frown. It is important to allow the patient to observe themselves in these expressions while in front of the mirror and to document pre-existing asymmetries of creases and muscle tone. After still photography is completed, a brief digital video clip should be taken of the same points of expression.
During this evaluation, it is important for the surgeon to understand different vectors of frowning and which muscle group may be contributing to the visible creases. provides a detailed analysis and description of these different muscle groups. The presence of oblique creases and horizontal creases indicate active medial depressors involving the oblique head of the corrugator, with the depressor supercillii muscle as well as the medial head of the orbicularis oculi muscle. The procerus muscle produces transverse dorsal nasal lines. Presence of vertical creases indicates a high level of activity of the transverse or lateral body of the corrugator muscle. These observations help the surgeon understand the dual innervation pattern of the glabellar complex. Understanding the neuroanatomy of the eyebrow muscles allows the surgeon to target the appropriate nerves with the GFX. The temporal branch of the facial nerve continues as lateral nerve to the transverse head of the corrugator supercilii and the angular nerve goes to the medial eyebrow depressor group and the procerus muscles as shown in Figure 3.2 .
Preparation
In preparation for the procedure, in selected cases, patients are provided with an oral analgesic and oral anxiolytic. The patient is positioned comfortably in a treatment chair so that the treating surgeon has access to both sides of the face as this is a bilateral procedure. After cleaning the facial skin with a standard prep solution, the skin is dried and specific markings are made on the skin surface ( Figure 3.3 ). It is helpful to mark out the depths of the frown lines as well as marking the lateral extent of the corrugator muscle. This is identified by asking the patient to squeeze the eyebrows together and a pen mark is placed at the lateral dimple that appears on the skin. This reference mark aids the surgeon’s judgment when the probe is being moved medially and encounters muscle tissue. At this point, and further medially, the distinction between nerve stimulation versus muscle stimulation can become more difficult. Another reference mark is made vertically on the forehead to mark the parasagittal plane of the midpupillary line. This surface marking limits the medial extent of any RF ablation so as to avoid injury to the main sensory neurovascular bundle which is a few millimeters more medial at the medial corneal limbus. For similar reasons, the inferior aspect of the midpupillary line is also marked on the lower eyelid skin to remind the operator of the infraorbital sensory nerve when ablations are performed for the angular nerve.