Flap |
Pedicle or free flap; distal or proximal pedicle |
Tissue |
Potentially innervated fasciocutaneous flap with little hair; also possible as a fascial flap |
Course of the vessels |
At the bottom of a fascial septum along the brachioradialis muscle as the leading structure |
Dimensions |
Maximum 8 × 20 cm |
Extensions and combinations |
Can be combined with a strip of brachioradialis or palmaris longus tendon, a bony segment of the radius, or a second proximal skin island based on a perforator vessel |
Anatomy |
|
Neurovascular pedicle |
— |
Artery |
Radial artery |
Veins |
Two concomitant veins or the cephalic system |
Length and arc of rotation |
Depends on flap location on the forearm; up to 15 cm |
Diameter |
Artery, 3–4 mm; veins, 3–5 mm (in the case of a free flap) |
Nerve |
Lateral antebrachial cutaneous nerve |
Surgical technique |
|
Preoperative examination and markings |
Identify the course of the radial artery by Doppler examination; Allen test |
Patient position |
Supine position with arm on arm board |
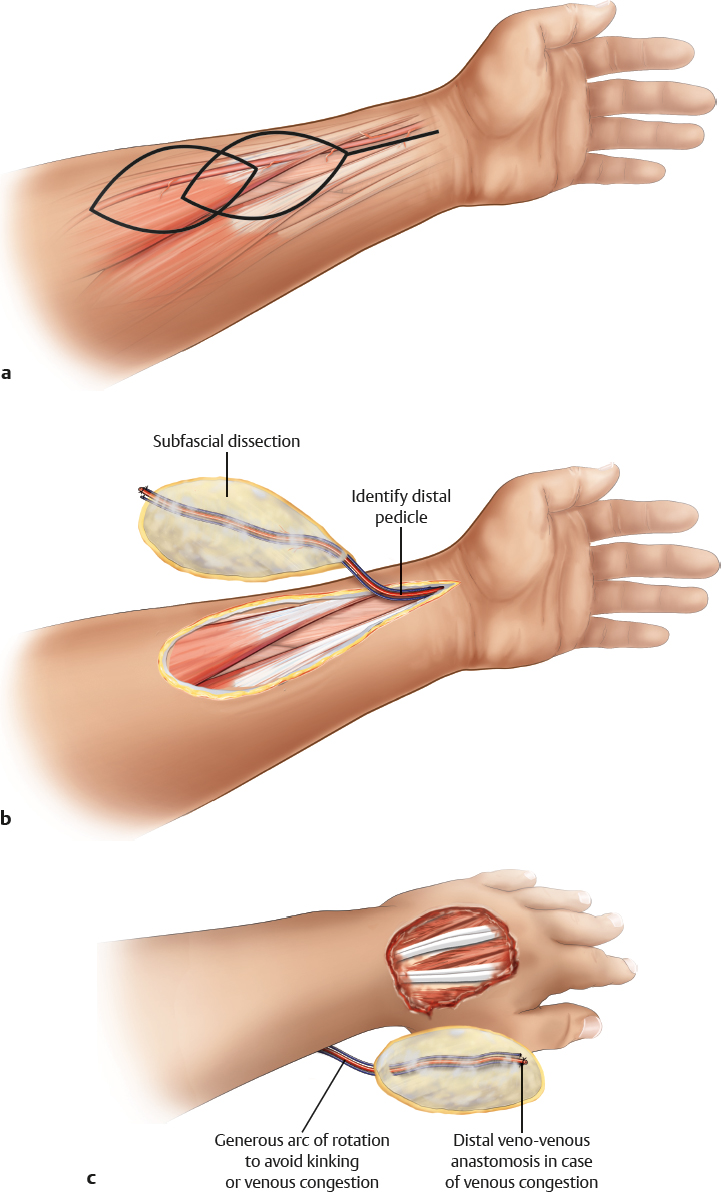
Dissection |
Mark the flap centered over the course of the vessel; incise the skin and make a subfascial dissection cuff toward the vessel; stay under the vessels and isolate the pedicle distally; include a cuff of subcutaneous fat and a subcutaneous vein if the flap is raised as a distal pedicle flap
For experienced surgeons, create a suprafascial dissection and a possible pedicle flap: raise flap from distal to proximal; isolate the vessels proximally; put a vessel clamp on the proximal pedicle; check for perfusion or signs of venous congestion; wait for 15 minutes; leave a subcutaneous vein long; ligate the proximal vessels and rotate the flap to the distal site; check again for perfusion and venous congestion; if the area is congested, connect the vein to a forearm vein (turbocharging)
Proximal pedicle: put a vessel clamp on the distal pedicle after isolating the flap; check perfusion; ligate the distal vessels |
Advantages |
|
Vascular pedicle |
A long, reliable pedicle with large-caliber vessels; atherosclerosis is rare; can be used as a “flow-through” flap when used as a free flap |
Flap size and shape |
Large flap; can be raised as a multi-island flap with strips of de-epithelialized subcutaneous tissue and fascia between the skin islands; many shapes possible; usually thin and pliable, even in obese patients |
Combinations |
Can be combined with extensions or second skin islands based on perforators, strips of tendons, and bony segments of the radius |
Dissection |
Donor and recipient sites can be dissected simultaneously |
Disadvantages |
|
Donor site morbidity |
Very conspicuous donor site with potential impairment of tendon function; indication has to be carefully weighed, especially in women; graft take can be impaired distally |
Pedicle |
Sacrifice of a major forearm artery |
Pearls and pitfalls |
|
Dissection |
Avoid separating the fascial septum from the vessels |
Extensions and combinations |
Maintain connections to bone and tendons when combined flaps are raised |
Contouring and correction |
Flap has only a little tendency to sag; contour corrections are rarely required |
Clinical applications |
Defects where flat, thin, and supple flaps are indicated; forearm, dorsum of the hand, and donor site appearance can be improved with suprafascial dissection |