FIGURE 17-1 Components of pulsed lavage with suction Irrigation fluid flows from the irrigation bag, through the tubing, into the handpiece, and through a central opening in the tip. As it is pulsed onto the wound bed, the contaminated fluid is suctioned through a concentric outer opening and into the tubing that goes to the suction canister. Setup of the equipment includes proper connection of all the tubing ends into the bag and the canister!
PLWS has been utilized in health care for decades beginning in the 1960s when US Army physicians first adapted modified WaterPik units for the irrigation of contaminated combat wounds.5,6,7,8 The original units have been advanced to the light-weight portable units that are currently used in both surgical irrigation and wound management in in-patient, outpatient, and home health settings.9 The gun-like shape of the handpiece makes the device easy to grip and maneuver and an assortment of tips adapt to different wound sizes and locations (FIGURE 17-2). While different vendors (BARD Davol, Inc, Warwick, RI; Stryker, Kalamazoo, MI; Zimmer, Inc, Warsaw, IN) market disposable PLWS units with different options, the basic equipment requirements are essentially the same (TABLE 17-1).

FIGURE 17-2 Photo of handpiece The pulsed lavage handpiece pulses sterile saline solution into the wound with a controlled psi and suctions the contaminated fluid into a closed suction container. Note how the therapist’s fingers are used to maintain good contact of the tip with the tissue. This helps prevent spillage and aerosolization of the fluid and directs the flow of the solution into the desired area. The system provides a sterile, closed system for irrigating open wounds in a variety of settings.
TABLE 17-1 PLWS Equipment Requirements
THEORY
PLWS delivers pulsed, pressurized irrigation at controlled pounds per square inch (psi) along with simultaneous removal or suction of contaminated irrigation fluid, thereby combining the benefits of both positive and negative pressure in one modality. Research supports that the combination of these pressure forces facilitates wound cleansing, debridement of slough, loosening of nonviable tissue, reduction of surface bacteria, increased local perfusion, and stimulation of granulation tissue.1,2,10
Positive Pressure
Positive pressure hydrotherapy for the management of open wounds can assist in general wound cleansing, debridement, and tissue stimulation (see TABLE 17-2). Whirlpool (WP) therapy, once considered the primary method of hydrotherapy,11 utilizes a turbine to generate positive pressure irrigation (FIGURE 17-3).1,3 However, with WP therapy, the psi created by the turbine at the wound surface has not been documented.11 Research supports that positive pressure hydrotherapy delivered at too low a psi can be ineffectual for wound cleansing and debridement; too high, and wound tissues are damaged and surface bacteria may be pushed deeper into the wound bed.12,13,14 For safe and effective delivery, the Agency for Health Care Policy and Research, the National Pressure Ulcer Advisory Panel, and the European Pressure Ulcer Advisory Panel recommend irrigation pressures for wound management stay between 4 and 15 psi.12,15 PLWS units are designed so that providers select known psi settings within the safe 4 to 15 psi range (FIGURE 17-4).
TABLE 17-2 Benefits of PLWS Positive Pressure

FIGURE 17-3 Photo of the whirlpool turbine provides positive pressure when agitating the water around a treatment area; however, the psi has not been determined The detrimental effects of treating extremities in a dependent position, inability to isolate wounds during treatment with concern for cross-contamination, and inability to treat patients who cannot be transported to hydrotherapy are just a few of the reasons that whirlpool is no longer considered the standard of care for the majority of wounds that need cleansing with irrigation.
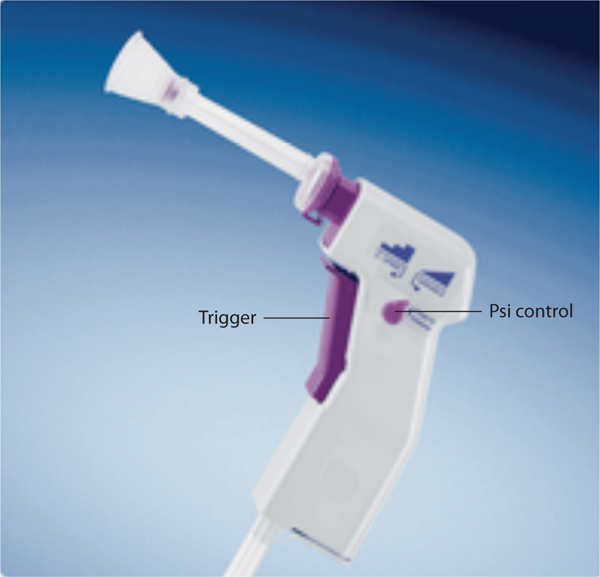
FIGURE 17-4 Photo of handpiece that shows the controls for psi PSI on this system is controlled by squeezing the trigger with the control turned to the left, toward the ramp (as shown in the picture). The pressure can also be “locked in” to low, medium, and high levels by turning the control to the left. (Davol, a Bard® Company. Davol is a registered trademark of C.R. Bard, Inc. Used with permission.)
Negative Pressure
Benefits associated with the negative-pressure component of PLWS are tissue stimulation, locally increased perfusion, reduction of surface bacteria,1 and removal of irrigation fluid (see TABLE 17-3). Research indicates that the suction force generated with the application of negative pressure stimulates granulation tissue proliferation and epithelialization through the process of cellular deformation and strain.2,10,16,17 Negative pressure also increases tissue perfusion by causing arterioles to dilate and thereby increasing local blood flow.2Increased perfusion supports granulation tissue formation and enhances the body’s ability to destroy and digest bacteria in the wound.18 PLWS also assists with reducing bioburden1,19 through the following mechanical means:
1. Debridement: the physical removal of loosened nonviable tissue and bacteria from the wound environment; removal of nonviable tissue also decreases food availability for remaining bacteria
2. Irrigation: removes microorganisms on the wound surface and in exudate as the irrigation fluid is evacuated
TABLE 17-3 Benefits of PLWS Negative Pressure
Bioburden may also be decreased by adding topical antibacterial medications to irrigation solutions.2,16 This can be especially beneficial in treating severely immunocompromised patients or patients with heavily contaminated, traumatic injuries with or without exposed bone.4 However, PLWS reduces surface bacteria primarily through mechanical means, and there is no promotion of bacterial resistance (an increasing concern as drug resistance increases) when normal saline alone is used as the irrigation fluid.20 Additionally, when using antibiotic irrigation solutions (eg, bacitracin), the potential for allergic reactions to those medications must be considered21 whereas normal saline has little to no allergic potential. The selection of antibacterial irrigation is based on systemic as well as local wound presentation.
Ms PL is a 34-year-old female who has had gastric bypass surgery for morbid obesity, followed by hernia repair with mesh reinforcement. She has a history of diabetes Type 2, which resolved after the bypass surgery. The hernia repair incision, located in the right lower abdomen, became necrotic, dehisced, and ultimately required surgical incision and drainage (I&D) to remove the infected tissue. The patient has been referred for wound care in preparation for surgical closure (FIGURE 17-5). The wound measures 18.5 cm × 12.7 cm × 3.8 cm deep, and connects to a smaller opening that is 3.6 cm × 1.7 cm.
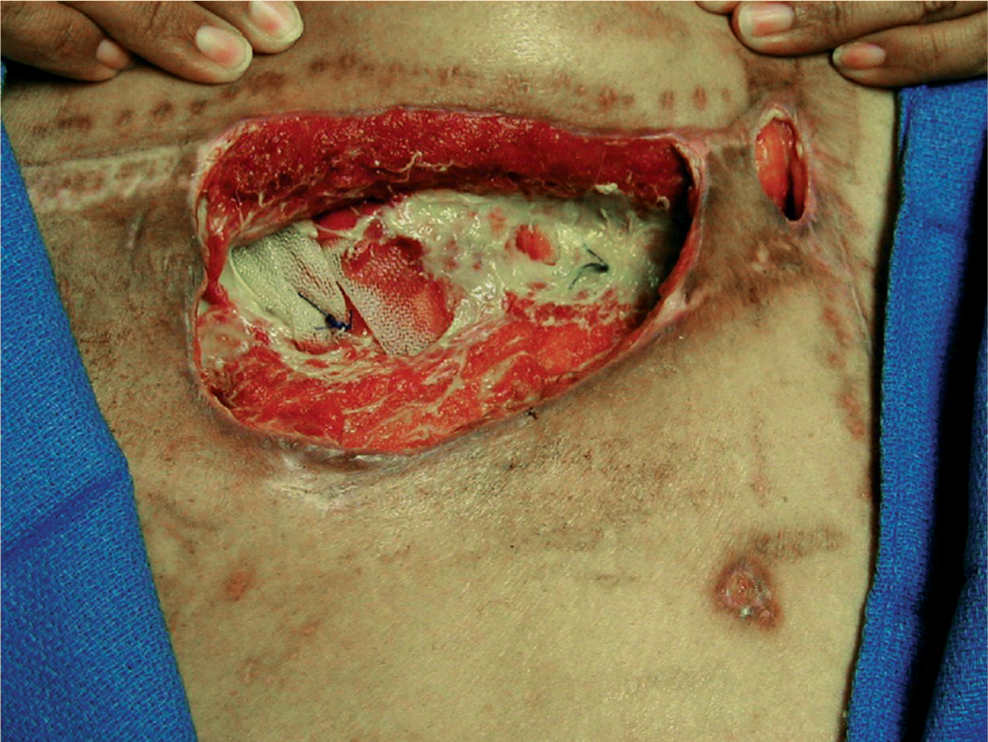
FIGURE 17-5 Photo of right lower abdominal wound on the patient who had dehisced incision after hernia repair Wound at time of evaluation was approximately 50% granulation, 25% slough and fibrous tissue, and 25% exposed mesh with moderate serosanguineous drainage.
1. What subjective and objective information do you need about this patient in order to develop a plan of care?
The systems review for this patient was negative for any cardiac, neuromuscular, or musculoskeletal issues. She was independent in all ADLs and IADLs, ambulatory at community level without a device. The wound measures 18.5 cm × 12.7 cm × 3.8 cm deep, and connects to a smaller opening that is 3.6 cm × 1.7 cm.
Drainage is moderate, tends to have a slight green tinge, but no odor after thorough cleansing.
Lab values of note: Hb1AC is 6.1, albumin is 2.2, hemoglobin is 10.4.
Medications: Vitamins per gastric bypass protocol. Patient has just completed a course of antibiotics (Vancomycin).
Social history: Patient lives with two daughters who are in school.
Patient goals:
1. To have surgical closure of wound as soon as possible
2. To return to work as a teacher’s aide
 Is pulsed lavage with suction an appropriate intervention for this patient?
Is pulsed lavage with suction an appropriate intervention for this patient?
 If so, describe the equipment and parameters you would use for optimal treatment.
If so, describe the equipment and parameters you would use for optimal treatment.
EFFECTS AT THE TISSUE AND CELLULAR LEVELS
The beneficial effects of PLWS have been discussed; however, full understanding of how PLWS facilitates healing at the cellular level requires further discussion. PLWS delivers positive pressure through pulsation of irrigation fluid. When a pulse of water strikes a tissue, the force of the pulse causes a brief compression of that tissue.4,8 Between pulses, target tissues decompress or recoil.4,8 PLWS produces multiple, rapid iterations of tissue compression-decompression cycles that mechanically dislodge bacteria,4,8,19 nonviable tissue, and debris from the wound bed. Adherent nonviable tissue remaining after a PLWS treatment is hydrated and loosened, thereby assisting natural phagocytosis.10 Hydration and loosening with PLWS is also an excellent method of preparing adherent nonviable tissue for sharp debridement. Compression-decompression mechanical manipulation also assists in exudate removal,10 which is especially important in chronic wounds since chronic wound fluid is damaging to wound tissues and contributes to delayed healing (FIGURE 17-6).17,18,23,24
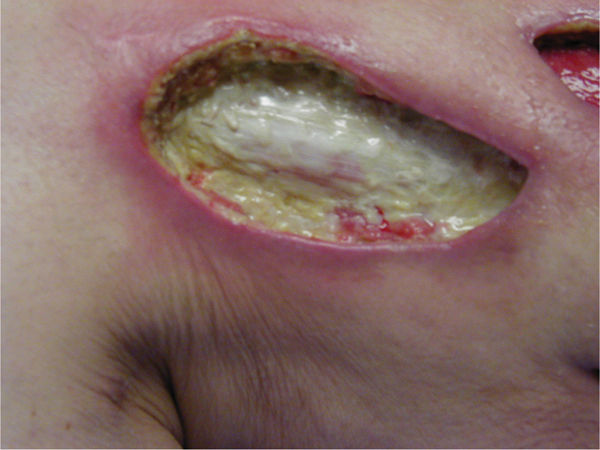
FIGURE 17-6 Wound with adhered fibrous tissue that can be loosened with PLWS, making selective debridement more effective PLWS also removes wound exudate containing chronic wound fluid components such as matrix metalloproteases (MMPs) that are detrimental to healing.
The negative-pressure component of PLWS also produces significant effects at the tissue and cellular levels via the mechanical stress10,17 or stretch18 on the structural components of extracellular matrix and local cells. This mechanical deformation17,18 has been shown to promote granulation tissue formation2 by stimulating increased protein synthesis by fibroblasts and by increasing cellular proliferation.10,18
Additionally, the warm irrigation fluids affect tissues by facilitating local increased vasodilation. Necessary components for tissue healing are delivered through the blood, and stimulating increased local blood flow delivers more leukocytes (white blood cells), antibodies, oxygen, and nutrients to the wound site.10 Increased local vasodilation also improves the delivery of systemic antibiotics to the area and increases the removal of toxic waste products.10
INDICATIONS
The use of PLWS is indicated for a variety of wounds that need atraumatic cleansing, debridement, tissue stimulation, and bacterial reduction (see TABLE 17-4) provided all precautions have been addressed. Specific etiologies that are appropriate for PLWS include wounds caused by neuropathy, pressure, venous insufficiency, and postsurgical incisional dehiscence or amputation healing by secondary intention.2 PLWS is also indicated for the removal of bacteria and debris in wounds associated with traumatic injury and bone exposure.4 Utilization of the flexible tips allows appropriate and safe use of PLWS for the irrigation and cleansing of tunnels, tracts, and undermining (FIGURES 17-7, 17-8).
TABLE 17-4 Indications for PLWS

Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


