The current melanoma staging system, as defined by the American Joint Committee on Cancer (AJCC), is the standard by which melanoma prognosis is determined. This article focuses on the components of the AJCC melanoma staging system regarding patient prognosis. In addition, this article summarizes the other commonly researched clinical and histologic melanoma prognostic factors and reviews the recent advancements in genetic biomarkers associated with prognosis.
- •
The AJCC melanoma staging system defines prognosis based on the standard TNM (tumor, regional nodes, distant metastasis) classification to create 4 (I–IV) clinical and pathologic stages.
- •
The tumor thickness serves as the main prognostic factor, with the mitotic rate and ulceration further subcategorizing the Breslow thickness to increase its prognostic accuracy.
- •
For advanced disease, the determination of lymph node involvement is the first step in evaluating for systemic involvement and predicting survivability.
- •
The AJCC has created an online melanoma prediction tool ( www.melanomaprognosis.org ) to more accurately determine melanoma prognosis for localized and regional disease.
- •
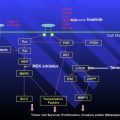
Research into identifying the major genetic pathways that contribute to the development of melanoma has created a new model to determine prognosis and develop new therapeutic options.
Introduction
The pioneering work by Drs Wallace H. Clark, Jr and Alexander Breslow established the framework for today’s melanoma prognosis models. Following the establishment of the Clark levels of invasion and the Breslow thickness in 1969 and 1970, respectively, Clark and colleagues, in 1989, described 6 independently predictive factors (mitotic rate, tumor-infiltrating lymphocytes, tumor thickness, anatomic site, patient sex, and histologic regression) that, when analyzed with tumor thickness, became the standard melanoma prognostic model. Today, the American Joint Committee on Cancer (AJCC) serves as the dominant staging system for melanoma, with the Breslow thickness being the principle component in determining outcomes. As medical science evolves into a genetic approach to understanding the balance between disease and health, research on genetic biomarkers has introduced an additional factor that influences prognosis. This article summarizes the current melanoma AJCC staging system and predictive model, discusses the more recent larger clinical studies and current reviews on common prognostic factors, and summarizes recent genetic biomarker development to understand the current staging system and future implications.
2009 AJCC melanoma staging and classification
The AJCC melanoma staging system defines prognosis based on the standard TNM (tumor, regional nodes, distant metastasis) classification to create 4 (I–IV) clinical and pathologic stages ( Tables 1 and 2 ). This classification system is pivotal because it unifies the staging nomenclature to predict the prognosis and determine the appropriate treatment.
| Classification | Thickness (mm) | Ulceration Status/Mitoses |
|---|---|---|
| T | ||
| Tis | NA | NA |
| T1 | ≤1.00 | a: Without ulceration and mitosis <1/mm 2 |
| b: With ulceration or mitoses ≥1/mm 2 | ||
| T2 | 1.01–2.00 | a: Without ulceration |
| b: With ulceration | ||
| T3 | 2.01–4.00 | a: Without ulceration |
| b: With ulceration | ||
| T4 | >4.00 | a: Without ulceration |
| b: With ulceration | ||
| N | Number of Metastatic Nodes | Nodal Metastatic Burden |
| N0 | 0 | NA |
| N1 | 1 | a: Micrometastasis a |
| b: Macrometastasis b | ||
| N2 | 2–3 | a: Micrometastasis a |
| b: Macrometastasis b | ||
| c: In-transit metastases/satellites without metastatic nodes | ||
| N3 | 4+ metastatic nodes, or matted nodes, or in-transit metastases/satellites with metastatic nodes | |
| M | Site | Serum LDH |
| M0 | No distant metastases | NA |
| M1a | Distant skin, subcutaneous, of nodal metastases | Normal |
| M1b | Lung metastases | Normal |
| M1c | All other visceral metastases | Normal |
| Any distant metastasis | Elevated | |
a Micrometastases are diagnosed after sentinel lymph node biopsy.
b Macrometastases are defined as clinically detectable nodal metastases confirmed pathologically.
| Clinical Staging a | Pathologic Stagingt b | ||||||
|---|---|---|---|---|---|---|---|
| T | N | M | T | N | M | ||
| 0 | Tis | N0 | M0 | 0 | Tis | N0 | M0 |
| IA | T1a | N0 | M0 | IA | T1a | N0 | M0 |
| IB | T1b | N0 | M0 | IB | T1b | N0 | M0 |
| T2a | N0 | M0 | T2a | N0 | M0 | ||
| IIA | T2b | N0 | M0 | IIA | T2b | N0 | M0 |
| T3a | N0 | M0 | T3a | N0 | M0 | ||
| IIB | T3b | N0 | M0 | IIB | T3b | N0 | M0 |
| T4a | N0 | M0 | T4a | N0 | M0 | ||
| IIC | T4b | N0 | M0 | IIC | T4b | N0 | M0 |
| III | Any T | N > N0 | M0 | IIIA | T14a | N1a | M0 |
| T14a | N2a | M0 | |||||
| IIIB | T14b | N1a | M0 | ||||
| T14b | N2a | M0 | |||||
| T14a | N1b | M0 | |||||
| T1-4a | N2b | M0 | |||||
| T14a | N2c | M0 | |||||
| IIIC | T1-4b | N1b | M0 | ||||
| T14b | N2b | M0 | |||||
| T14b | N2c | M0 | |||||
| Any T | N3 | M0 | |||||
| IV | Any T | Any N | M1 | IV | Any T | Any N | M1 |
a Clinical staging includes microstaging of the primary melanoma and clinical/radiologic evaluation for metastases. By convention, it should be used after complete excision of the primary melanoma with clinical assessment for regional and distant metastases.
b Pathologic staging includes microstaging of the primary melanoma and pathologic information about the regional lymph nodes after partial (ie, sentinel lode biopsy) or complete lymphadenectomy. Pathologic stage 0 or stage IA patients are the exception; they do not require pathologic evaluation of their lymph nodes.
The T classification describes the state of the primary tumor by the thickness, presence of ulceration, and mitotic rate. The N designation signifies the degree of regional lymph node involvement subcategorized by microscopic and macroscopic disease, and the M category defines the presence and location of distant metastatic disease. The current melanoma TNM classification system is predominantly an anatomic and pathologic staging system; the Breslow thickness continues to be the main prognostic factor. The 2009 classification introduced a few significant modifications to the 2002 classification ( Table 3 ). The mitotic rate in the T category replaces the Clark level of invasion in the 2009 staging system and the integration of immunohistochemical tumor detection with no lower tumor threshold in the N category has also been added. The AJCC’s prognosis determinations were based on a multivariate analysis, using the Cox proportional hazards model, of prospective data on 30,946 patients with stages I, II, and III melanoma and 7972 patients with stage IV disease in the AJCC melanoma staging database. Survival curves were created through the Kaplan-Meier product-limit method and compared using the log-rank test.
| Factor | Sixth Edition Criteria | Recommended Seventh Edition Criteria | Comments |
|---|---|---|---|
| Thickness | Primary determinant of T staging | Same | Thresholds of 1.0, 2.0, and 4.0 mm |
| Level of invasion | Used only for defining T1 melanomas | Same | Used as a default criterion only if mitotic rate cannot be determined |
| Ulceration | Included as a secondary determinant of T and N staging | Same | Signifies a locally advanced lesion; dominant prognostic factor for grouping stages I, II, and III |
| Mitotic rate per square millimeter | Not used | Used for categorizing T1 melanoma | Mitosis ≥1/mm 2 used as a primary criterion for defining T1b melanoma |
| Satellite metastases | In N category | Same | Merged with in-transit lesions |
| Immunochemical detection of nodal metastases | Not included | Included | Must include at least 1 melanoma-associated marker (eg, HMB-45, Melan-A, MART-1) unless diagnostic cellular morphology is present |
| 0.2 mm threshold of defined N+ | Implied | No lower threshold of staging N+ disease | Isolated tumor cells or tumor deposits <0.1 mm meeting the criteria for histologic or immunohistochemical detection of melanoma should be scored as N+ |
| Number of nodal metastases | Primary determinant of N staging | Same | Thresholds of 1 v 2–3 v 4+ nodes |
| Metastatic volume | Included as a second determinant of N staging | Same | Clinically occult (microscopic) nodes are diagnosed at sentinel node biopsy v clinically apparent (macroscopic) nodes diagnosed by palpation or imaging studies or by the finding of gross (not microscopic) extracapsular extension in a clinically occult node |
| Lung metastases | Separate category as M1b | Same | Has a somewhat better prognosis than other visceral metastases |
| Elevated serum LDH | Included as a second determinant of M staging | Same | Recommend a second confirmatory LDH level if elevated |
| Clinical vs pathologic staging | Sentinel node results incorporated into definition of pathologic staging | Large variability in outcome between clinical and pathologic staging; sentinel node staging encouraged for standard patient care should be required before entry into clinical trials |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


