Profunda Artery Perforator Flap for Breast Reconstruction
Katie E. Weichman
Nicholas Haddock
DEFINITION
The profunda artery perforator (PAP) flap is a variation of the posterior thigh myocutaneous flap, which was initially described by Hurwitz1 and further popularized for reconstruction of burn contractures, pressure sores, and extremity wounds.2,3 Since its description by Allen et al. in 2010, it has been recently popularized for use in breast reconstruction.4
Although abdominally based free flaps remain the most common choice for breast reconstruction secondary to sufficient skin and soft tissue, patients may require alternative donor sites for various reasons. These reasons include lack of abdominal donor site secondary to prior abdominal surgery or abdominoplasty, inadequate volume in the abdomen, and patient preference.
ANATOMY
The profunda femoris artery originates from the common femoral artery. It runs deep in the thigh and between the pectineus and the adductor longus and on the posterior side of the adductor longus.
The profunda femoris artery gives off several branches including lateral circumflex femoral artery, medial circumflex femoral artery, and several perforating branches that perforate the adductor magnus muscles to the posterior and medial compartments of the thigh.
There are typically three to four perforating arteries originating from the profunda femoris.
First perforating artery passes posteriorly between the pectineus and adductor brevis and then pierces the adductor magnus close to the linea aspera.
Second perforating artery larger than the first pierces the tendons of the adductor brevis and adductor magnus and divides into anterior and posterior branches.
Third perforating artery is given off below the adductor brevis, and it pierces the adductor magnus and divides into branches that supply posterior femoral muscles.
The perforating vessels used in the PAP flap have been evaluated in imaging studies based on both size and location and perfusion.
The perforator is consistently found in the upper medial thigh posterior to the gracilis. The most common location of the perforator in the medial thigh is exiting the fascia in the vicinity of the adductor magnus about 3.8 cm from the midline and 5.0 cm below the gluteal fold. The second most common perforator location is in the vicinity of the biceps femoris and vastus lateralis at 12 cm from the midline and 5.0 cm below the gluteal fold5 (FIG 1).
The thigh has three compartments: anterior compartment, medial compartment, and posterior compartment. The medial and posterior compartments are highlighted for profunda artery flap dissection (FIG 2).
The medial compartment includes the obturator externus muscle, gracilis muscle, adductor longus muscle, adductor brevis, and adductor magnus.
Gracilis muscle
Origin: The line on the external surfaces of the body of the pubis, inferior pubis ramus, and the ramus of the ischium
Insertion: Medial surface of proximal shaft of the tibia
Action: Adducts the thigh at the hip and flexes the knee
Arterial supply: Medial femoral circumflex
Innervation: Obturator nerve
Adductor longus
Origin: External surface of the body of the pubis (triangular depression inferior to pubic crest and lateral to pubic symphysis
Insertion: Linea aspera to middle one-third of the shaft of the femur
Action: Adducts and medial rotates the thigh at the hip
Arterial supply: Profunda femoris
Innervation: Obturator nerve
Adductor magnus
Origin: Ischiopubic ramus
Insertion: Posterior surface of the proximal femur, linea aspera, and medial supracondylar line
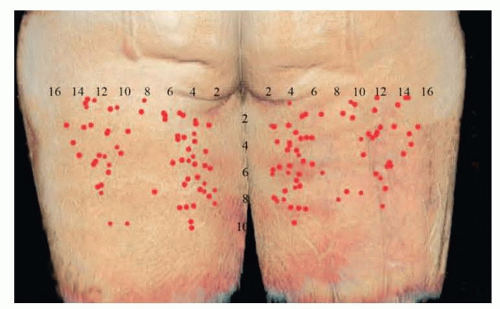
FIG 1 • Posterior thigh perforator location based on CT scanning. Described as location from the gluteal fold and from the midline.
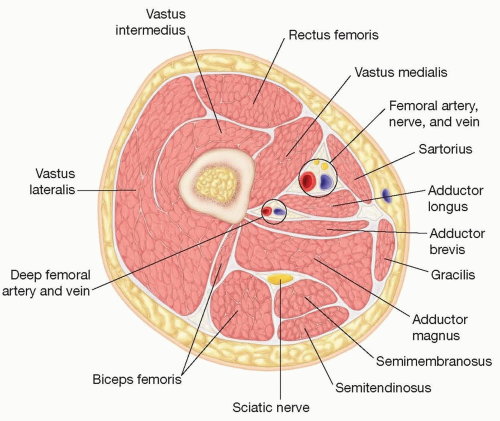
FIG 2 • Cross section of the thigh at the level of the profunda artery perforators.
Action: Adducts and medially rotates the thigh at hip joint
Arterial supply: Profunda femoris
Innervation: Obturator nerve
The posterior compartment has three muscles: biceps femoris, semitendinosus, and semimembranosus.
Biceps femoris
Origin—long head: Ischial tuberosity
Origin—short head: Linea aspera on posterior surface of the femur
Insertion: Both insert onto the head of the fibula as a single tendon.
Action: Flexion at the knee and extends the hip
Arterial supply: Profunda femoris artery and perforators of profunda femoris artery
Innervation: Sciatic nerve
Semitendinosus
Origin: Ischial tuberosity of the pelvis
Insertion: Medial surface of the tibia (pes anserinus)
Action: Flexes the leg at the knee joint and extension of the hip
Arterial supply: Inferior gluteal artery and perforating arteries from the profunda femoris
Innervation: Sciatic nerve (tibial portion)
Semimembranosus
Origin: Ischial tuberosity
Insertion: Medial tibial condyle
Action: Flexion of the leg at the knee joint and extension of the hip
Arterial supply: Profunda femoris and gluteal arteries
Innervation: Sciatic nerve (tibial portion)
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients present for evaluation for either delayed or immediate breast reconstruction.
This includes patients with a history of breast cancer, patients undergoing prophylactic mastectomy, patients with congenital abnormalities, and transgender patients.
Physical examination includes examination of the abdomen and posteromedial thighs to assess availability of excess tissue.
Timing of reconstruction should be planned in patients with prior history of breast irradiation. The authors prefer to wait 6 months after the completion of radiation therapy prior to completing delayed reconstruction.
Smoking status is also assessed.
Additionally, tamoxifen should be held 2 weeks prior to surgery and 2 weeks after surgery.
IMAGING
Patients considering PAP flap reconstruction should undergo preoperative imaging with either computed tomography angiogram (CTA) or magnetic resonance angiography (MRA) of the pelvis and lower extremity.
Imaging is performed in the supine position and coordinated with the radiologist for appropriate evaluation of images.
Perforators should be described as they exit the deep muscular fascia and described based on location in an x–y axis. The gluteal fold will be set as zero on the y-axis, and the posterior border of the gracilis will be set as zero on the x-axis (FIG 3).
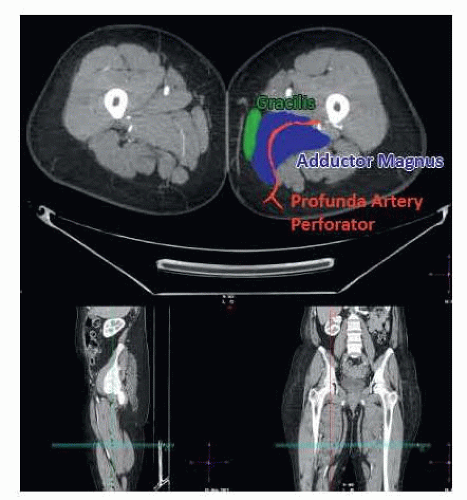
FIG 3 • CTA of the lower extremity identifying the location of the profunda artery perforator behind the gracilis traversing the adductor magnus toward the profunda femoris artery.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access