This chapter presents the principles and basic steps of the senior author’s operative technique for implant augmentation of the facial skeleton.
Preparation
In anticipation of implant surgery, steps to minimize the likelihood of infection are taken. To facilitate intraoperative hemostasis, patients are instructed to discontinue any medications or foods that compromise the blood clotting system. To optimize intraoral hygiene, a professional dental examination and cleaning may be indicated. Patients are always prescribed chlorhexidine mouthwash for 48 to 72 hours prior to the anticipated surgery.
Anesthesia
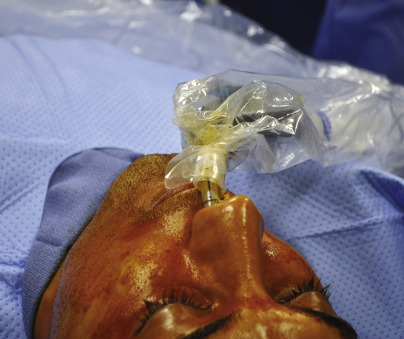
With the exception of chin augmentation, operations are performed with the patient under general anesthesia, preferably nasotracheal anesthesia. Since most operations employ intraoral incisions, this approach optimizes access and allows optimum preparation of the operative site as well as control of the airway ( Fig. 4.1 ). The operative field is infiltrated with a solution containing bupivacaine (Marcaine) and epinephrine (1:200,000), for immediate postoperative pain relief and to optimize intraoperative hemostasis. Both the skin and the oral mucosa are prepared with a povidone-iodine solution. Antibiotics, usually cephalosporins, are administered intravenously prior to the onset of surgery and intraoperatively depending on the length of surgery. Oral antibiotics are administered for the 5 days following surgery only if intraoral access for implant placement was employed.
Incisions
Incisions are borrowed from craniofacial and aesthetic surgery. They are always made through intact skin remote from implant placement. Implants positioned directly beneath surgical incisions are at risk for exposure, contamination and then, implant loss.
Coronal incisions are used to place implants in the frontal and temporal areas. Transconjunctival retroseptal incisions (often with a lateral canthotomy for increased exposure) are used to access the infraorbital rim, malar area, and internal orbit. The lateral extent of the lower lid blepharoplasty incision provides access to the lateral orbit and zygomatic arch. This small cutaneous incision leaves an inconspicuous scar. It is used with the transconjunctival approach when a lateral canthotomy is avoided. Blepharoplasty skin–muscle flaps provide alternative access to this area.
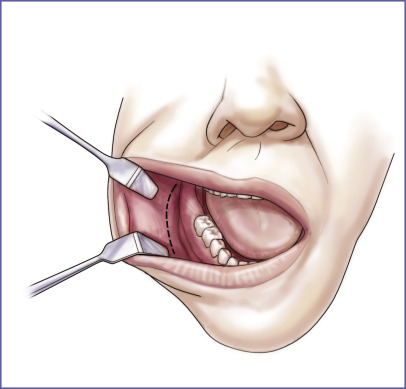
Intraoral incisions are used to augment the midface as well as the mandibular body and ramus. Intraoral incisions are made with a generous labial cuff to allow watertight, reliable mucosal closure ( Fig. 4.2 ).
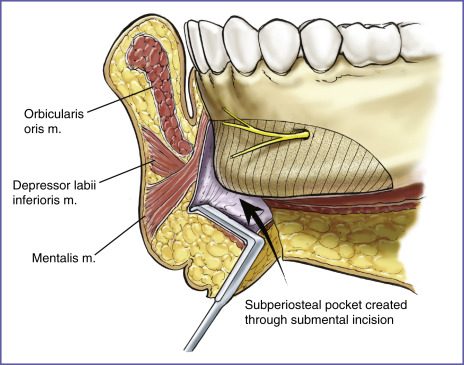
Chin area augmentation is preferably performed through submental incisions ( Fig. 4.3 ). Submental approaches to the chin provide optimal exposure of the skeletal anatomy and the mental nerves. Unlike the intraoral approach, which avoids a cutaneous scar, the submental approach does not violate the mentalis muscle. Mentalis dysfunction can result in lower lip descent, excessive lower tooth show, and chin pad ptosis.
Exposure
The area to be augmented is exposed widely in the subperiosteal plane. Wide subperiosteal exposure is important for several reasons. It allows accurate identification of the area to be augmented and important adjacent structures. This exposure prevents iatrogenic damage and provides landmarks for orientation and hence, symmetric implant positioning. Wide exposure also allows easy access for screw immobilization of the implant and its final in-place contouring. The resultant soft tissue mobilization also allows tension-free closure of the access incision ( Fig. 4.3 ).
This technique differs significantly from tradition whereby dissection of only the area to be augmented was advocated. The resultant small pocket was intended to prevent postoperative implant migration. A limited dissection is possible for placement of smooth-surfaced implants but is not possible for the placement of porous implants to which soft tissues tend to adhere (like Velcro), making placement more difficult.
Wide subperiosteal exposure of the area to be augmented optimizes accuracy of implant placement.
Implant Selection
The senior author prefer porous polyethylene implants (Omnipor, Matrix Surgical, Atlanta, GA; Medpor, Stryker, Kalamazoo, MI), to augment the facial skeleton.
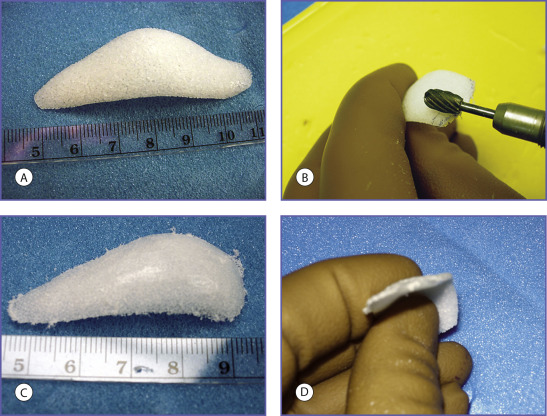
Porous polyethylene is firm and flexible. It is easily carved with a scalpel or contoured with a rasp or motorized burr. It is best immobilized and applied to the skeleton with screws. It can be molded to the external contours of the skeleton by heating it in hot water, an attribute that the author utilizes infrequently.
The favorable biocompatibility of this implant material can also be attributed to its porous surface. Porous polyethylene has pores of sufficient size to allow fibrous tissue ingrowth and relative host incorporation, as opposed to the host encapsulation observed with smooth-surfaced implants. Porous polyethylene has a continuous system of inner connecting pores approximately 125 to 250 μm in diameter. Animal studies have demonstrated that pore sizes of more than 100 μm encourage tissue ingrowth, whereas pore sizes of less than 100 μm limit the extent of tissue ingrowth. Materials with pore sizes greater than 300 μm have drawbacks associated with material breakdown. Clinical specimens have demonstrated rapid ingrowth of fibrous tissue after human implantation. Rather than the dense connective tissue capsules observed with smooth-surfaced implants, porous polyethylene implants exhibit a thin connective tissue membrane that is contiguous with the ingrown tissue. It has been noted during revision operations that fibrous tissue ingrowth can be sufficient to result in bleeding when the implants are modified in situ with a scalpel, and in certain circumstances, ingrowth exhibits sufficient vascularity to allow skin grafts to be placed directly over the implant.
Fibrous tissue ingrowth improves the biocompatibility of porous implants because it limits their movement. Movement is an essential factor in determining the host response to an implant. Because the host foreign body reaction encapsulates smooth-surface implants, a smooth implant never binds to the host bed and therefore is predisposed to move. Encapsulation of smooth implants and their subsequent predisposition to movement are directly or indirectly responsible for the majority of the late complications observed with smooth implants. When used to augment the chin, smooth silicone implants are known to cause significant bone resorption, which is attributed to implant motion caused by the overlying mentalis muscle. Bone erosion is not clinically significant unless an implant and the subsequent erosion overlies a tooth root. Animal studies have demonstrated that porous implants result in less bone resorption than do smooth implants. Bikhazi and Van Antwerp, in a prospective cephalometric study of five patients undergoing chin augmentation with porous polyethylene implants, did not observe bone resorption beneath the implants. When this author has removed cheek implants at 6 months and chin and mandibular implants at 1 year, the erosion was barely perceptible.
The use of porous implants has been criticized because, unlike smooth implants, they require wider exposure for positioning and are more difficult to remove. Personal preference and the “learning curve” have made both of these problems less significant. Wider exposure has resulted in more accurate implant positioning. Because the initial augmentation has been more satisfactory for the majority of patients, revision surgical procedures have been infrequent. When porous polyethylene implants require removal, dissection directly on the implant minimizes adjacent soft tissue trauma. The absence of a thick fibrous capsule allows the soft tissues to collapse after implant removal, permitting restoration of the preimplant contour. This is not always the case after silicone implant removal, where the fibrous capsule maintains the contour of the implant.
It is important to note that the manufacturer provides multiple implant shapes and sizes intended for specific anatomical areas. It is unusual for the senior author to use an implant without changing its contour (reducing it) to meet the needs of the specific situation ( Fig. 4.4 ).