(1)
Klinik für Plastische Gesichtschirurgie, Marienhospital Stuttgart, Stuttgart, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-662-49706-7_5) contains supplementary material, which is available to authorized users.
Keywords
Reduction rhinoplastyCompound techniqueComponent techniqueSpreader flap techniqueSpreader graft techniqueOsteotomiesDorsal camouflage5.1 Surgical Principles
Most patients seeking rhinoplasty desire enhancements of their nasal profiles. In fact, more than 80 % of all rhinoplasty patients are seeking a reduction rhinoplasty because they feel their nasal profiles are too prominent. However, it is first necessary to determine why the patient feels this way, since there are many different causes of the overly prominent nose. Proper characterization is critical, since failure to correctly analyze the cosmetic deformity may lead to inappropriate treatment and patient dissatisfaction. Is the problem a simple overprojected dorsal hump? Or is the entire nasal profile, including the nasal tip, overprojected (i.e., rhinomegaly)? Alternatively, does the excessive prominence result from a tension-nose deformity in which an overprojected dorsal septum gives rise to pinching of the middle vault and excessive elongation of the nostrils (Fig. 5.1)?
The typical nasal hump is a combination of an overprojected cartilaginous dorsum and an overprojected bony dorsum. On the other hand, overprojection can be restricted to either the bony or the cartilaginous segment. The latter is known as an idiopathic parrot-beak deformity.
For surgical reduction of the nasal dorsum, different treatment options are available. However, regardless of the method chosen, nasal mucosa should first be elevated from the undersurface of the cartilaginous hump to expose the junction of the upper lateral cartilages and the dorsal septum. This enables a so-called extramucosal dissection, which preserves the protective mucosal barrier and stabilizes the overlying graft material. Additionally it minimizes contracture following hump resection. We perform dorsal reduction in most cases using the open approach. We first begin by dividing the membranous septum in order to expose the leading edge of the caudal septum. We then elevate the outer perichondrium off the inner perichondrium. Histologic analysis of the septal mucosa has identified two layers of perichondrium (Pirsig and Fischer 1982). The inner layer is tightly adherent to the cartilage matrix, whereas the outer layer is more easily elevated for flap dissection. We denude the septal cartilage of the outer perichondrium, which provides a comparatively bloodless plane of dissection and tends to produce fewer lacerations in the septal flaps. The extramucosal dissection can then be performed easily after entering the correct plane, for example, by using a suction dissector (Fig. 5.2). The instrument we are using for this purpose was developed by Haraldsson (Medicon eG, Tuttlingen, Germany); it has a semisharp tip and a revolving handle. This instrument enables us to safely and quickly dissect the mucosa, even without direct visualization.
For many years, we have been using a compound (or en bloc) resection technique for hump removal (Fig. 5.3). The cartilaginous hump was transected at the desired height using a no. 11 blade, beginning caudally at the distal margin of the hump and ending cephalically at the bony cartilaginous junction. The left upper lateral cartilage was then transected, followed by the dorsal septum and the right upper lateral cartilage. After all three components of the cartilaginous hump have been cut, we inserted a sharpened chisel into the newly made gap and engaged the lower end of the bony hump. Once the proper trajectory has been confirmed, we transected the bony hump and completed the en bloc resection. We preferred not to use an osteotome for bony hump resection since osteotome movement is more likely to result in inadvertent overresection of the nasal bone. Overresection is less likely with a sharp chisel with a long flat blade that cuts like a knife (Fig. 5.4). However, it is important to sharpen the blade before each use because it dulls easily. A major advantage of the compound resection technique is the comparatively large block of composite tissue that is generated by hump removal. When necessary, the resected hump can be remodeled and reshaped using a power drill to create an onlay graft, which is ideal for refinement of the dorsum. The graft can be used to cover minor contour irregularities or to conceal an open roof deformity (Fig. 5.5). The major disadvantage of this technique is resection of the ULC where it is fused to undersurface of the bony hump. By resecting a tall bony hump, a bony cartilaginous open roof may be created potentially causing irregularities in the surface contour of the rhinion.
As an alternative to the en bloc method, the component technique can be used for dorsal hump resection. Because of its ease and precision, it has become our preferred technique for hump removal (Fig. 5.6). After completing the extramucosal dissection, we divide the upper lateral cartilages from the dorsal septum and treat each anatomic component of the cartilaginous dorsum separately (i.e., a split technique). First we lower the dorsal septum using a straight scissors. Unless we are planning to reconstitute the middle vault with spreader flaps, each upper lateral cartilage is then trimmed individually with a straight scissors prior to spreader graft placement. When using spreader flaps, the upper lateral cartilages are bluntly detached from the undersurface of the nasal bones prior to bony hump resection. Typically, there is a 10- or 12-mm overlap.
The next step in the component technique is resection of the bony dorsum. Often, the bony hump is much smaller than expected, since the bony contribution to the dorsal hump is usually only 5–8 mm in length. Therefore, in most cases we prefer reducing the bony hump with a rasp rather than with a chisel. At present we prefer a rasp with disposable blades (Fig. 5.7) so that a sharp instrument is always available. Only with very large and thick humps is our algorithm changed, and the hump is removed using a chisel.
Transection of the dorsal hump is then followed by osteotomies to remodel the nasal pyramid. Osteotomies can be classified according to their shape: curved or straight. Curved osteotomy cuts are commonly used for paramedian osteotomies that diverge or “fade” laterally at their upper ends, often to join curved lateral osteotomy cuts that have either a high-to-low-to-high or a low-to-high configuration (Fig. 5.8). However, we prefer straight osteotomies, which yield larger bony fragments for more effective bone contouring. Therefore, we perform a straight paramedian osteotomy, a straight transverse osteotomy, and a straight low-to-low lateral osteotomy as our standard technique (Fig. 5.8). The paramedian osteotomy is performed using a power-driven Lindemann fraise, beginning inferiorly and extending superiorly to create precise parasagittal cuts parallel to the septum. By using a fraise, we can also remove additional bone to create a small open roof in order to prevent blocking of the fragments during infracture. Hence, the Lindemann fraise facilitates both precise placement of straight paramedian osteotomies and narrowing of the central bony complex to optimize infracture (Fig. 5.9). This process is followed by the transverse and the low-to-low lateral osteotomy, which are always performed percutaneously (Fig. 5.10). Two percutaneous skin incisions are required, one vertically oriented at the junction of the caudal and middle thirds and one transversely oriented at the junction of the cranial and middle thirds. For this procedure, we use a 2- or 3-mm unguarded osteotome. After inserting the instrument through the skin incision, we use the osteotome to elevate the soft tissues along the osteotomy line in order to displace the vessels and reduce bleeding (Fig. 5.11).
Based upon our experience, the percutaneous technique minimizes bone fragmentation by optimizing angulation of the osteotome. Although the osteotomy lines converge near the inner canthus, we prefer not to join the osteotomy cuts. Instead, we use a greenstick fracture with manual pressure to complete the release and mobilization of the nasal bones.
The next step is internal nasal valve reconstruction. In most cases we use a spreader flap technique (. see Fig. 5.11). Spreader flaps are created from upper lateral cartilage that remains after cartilaginous (septal) hump resection. The overprojecting edges of the upper lateral cartilage are scored or nonscored, invaginated inward, and then sutured flush to the newly established dorsal septum. We favor this technique over the use of spreader grafts, since it creates a very smooth dorsum as well as a favorable internal nasal valve configuration. Furthermore, spreader flaps typically produce good aesthetic dorsal lines.
Another option for internal valve reconstruction is the use of spreader grafts (Fig. 5.12). However, like spreader flaps, spreader grafts are also used to contour the middle vault, reinforce a weak dorsal septum, or compensate for middle vault asymmetries. Spreader grafts can be created from the previous septal dorsum or from central parts of the quadrangular cartilage. Care must be taken to bridge the keystone area because this is the most sensitive part of the dorsum. Typically, spreader grafts have a width of 1–2 mm and a height of approximately 3 mm. Fixation to the dorsal septum is accomplished by means of horizontal mattress sutures, which are recessed to permit additional smoothing of the cartilaginous dorsum when needed. Following spreader graft fixation, the upper lateral cartilages are trimmed flush with the dorsal septum and sewn to the newly created dorsal construct.
The last step of this procedure is smoothing the dorsum. For the bony dorsum, this can be accomplished with a power drill to eliminate any contour irregularities. Smoothing the bony cartilaginous junction or the cartilaginous dorsum is accomplished with a no. 11 blade. The benefits of spreader flaps or spreader grafts are many. These include maintaining or improving internal valve patency and/or straightening the cartilaginous dorsum. Pinching of the upper lateral cartilages adjacent to the bony/cartilaginous junction—the so-called inverted-V deformity—is also reversed and/or prevented using spreader flaps or spreader grafts. The by-products of these corrections are smooth and symmetrical and have continuous dorsal aesthetic lines.
Depending upon the desired cosmetic objective, the dorsum can be intentionally overreduced if immediate dorsal augmentation is preplanned. In our hands, augmentation of the dorsum is accomplished by reimplantation of a surgically modified (composite) dorsal hump or by blanketing the nasal bridge with one or two layers of autogenous or allogenic fascia (TutoplastR; Tutogen Medical GmbH; Neunkirchen am Brand, Germany) (Fig. 5.13). In order to create a smooth and even dorsal contour, full-length onlay grafts are preferable. In the case of an underprojected nasion, which is a common contour deficiency, we prefer to avoid isolated radix grafts—which often produce step-off deformities—and use full-length fascial grafts instead.
For some time, our first choice of refining the dorsal contour has been free diced cartilage. All residual cartilage remnants are finely diced into a paste-like consistency and injected using a plain tuberculin syringe. The injected material is then gently molded with digital pressure until the desired contour is achieved. After contouring is complete, the dorsum is stabilized with an outer layer of adhesive tape prior to final closure of marginal incisions (Fig. 5.14).
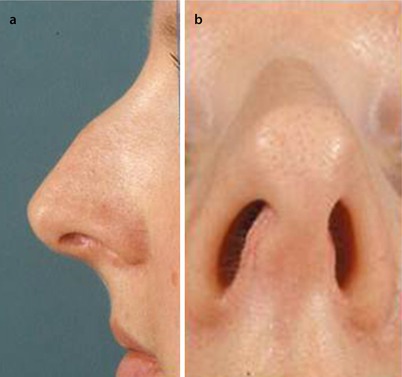
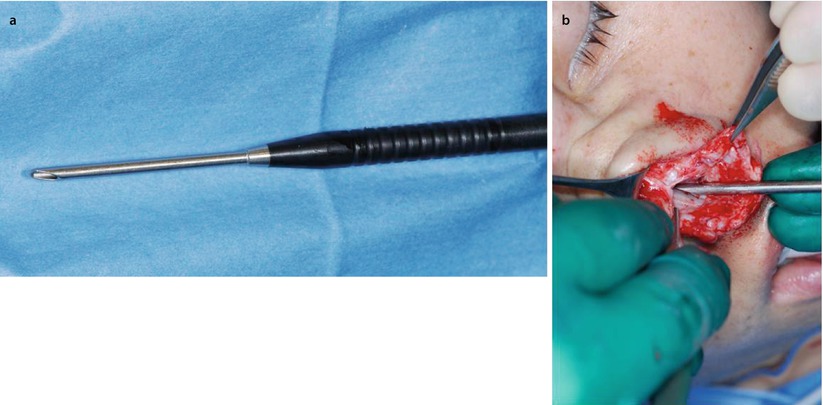

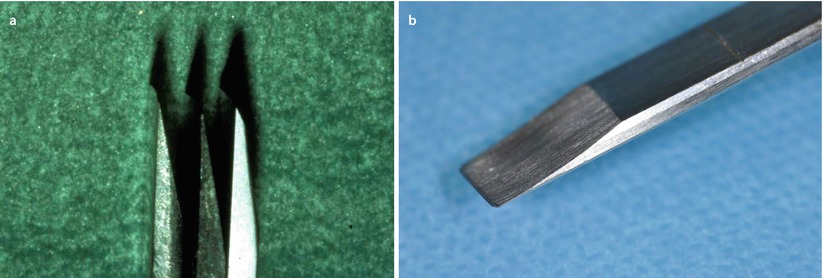
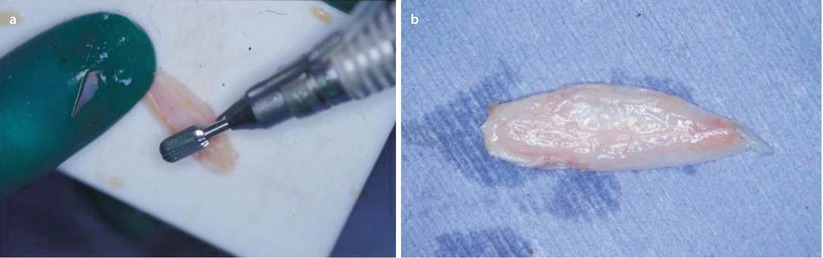




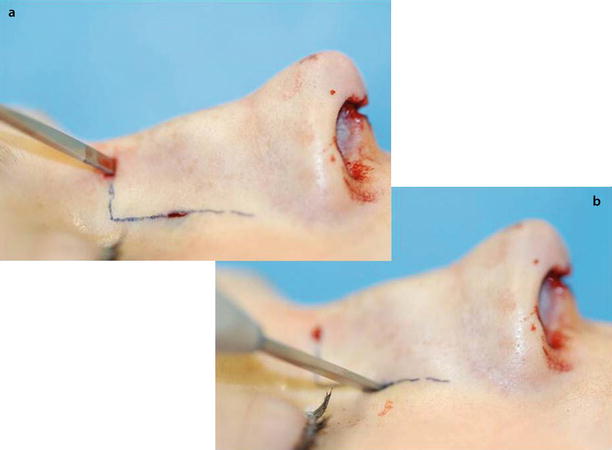
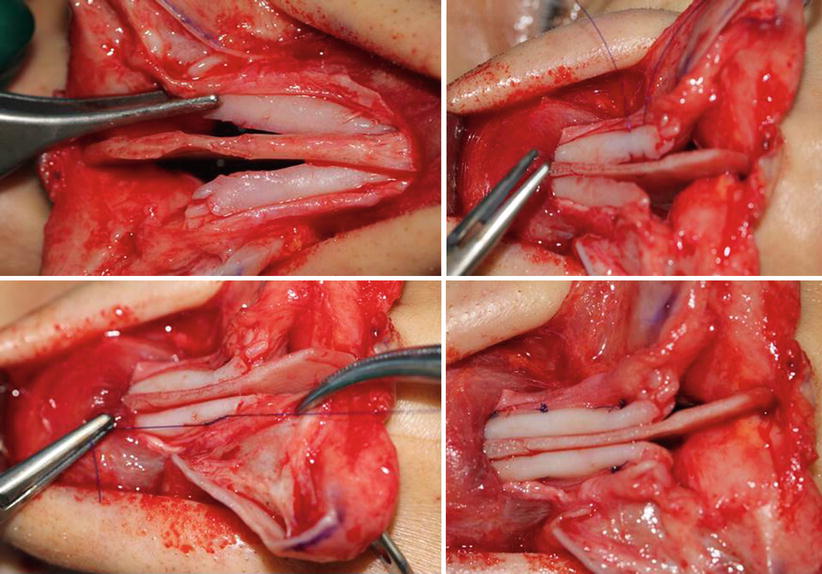

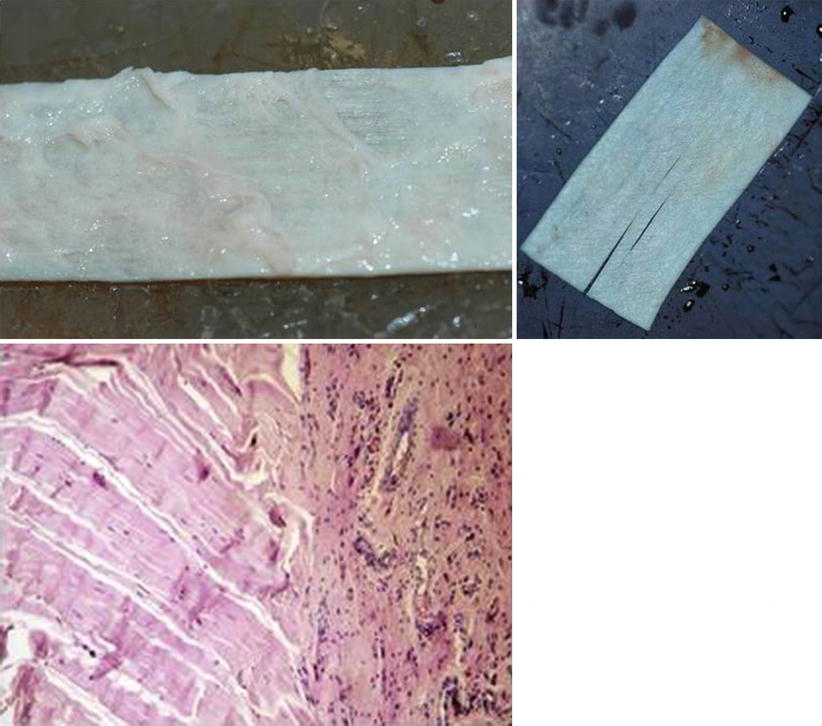

Fig. 5.1
(a, b) Tension nose with elongated nostrils
Fig. 5.2
(a, b) Suction dissector with revolving handle
Fig. 5.3
(a, b) En bloc hump resection
Fig. 5.4
(a, b) Chisel with long flat blade
Fig. 5.5
(a, b) Surgically modified hump for reinsertion as a dorsal onlay graft
Fig. 5.6
(a–d) Component hump resection
Fig. 5.7
Manual rasp with disposable blades
Fig. 5.8
Planning of the osteotomies
Fig. 5.9
(a, b) Using Lindemann fraise for paramedian osteotomy
Fig. 5.10
(a, b) Small osteotome inserted through a percutaneous incision
Fig. 5.11
Spreader flap technique
Fig. 5.12
Spreader graft technique
Fig. 5.13
Allogenic fascia lata (Tutoplast)
Fig. 5.14
Finely diced cartilage in tuberculin syringe for camouflaging irregularities
5.2 Case Studies
5.2.1 Case 1: Minor Hump Reduction with Power Drill
A 27-year-old female presented with a narrow and overprojected dorsum complaining of left-sided nasal obstruction. Endonasal examination showed a central septal deviation in the left nasal passage. The tip was also bulbous and slightly asymmetrical.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


