(1)
Klinik für Plastische Gesichtschirurgie, Marienhospital Stuttgart, Stuttgart, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-662-49706-7_7) contains supplementary material, which is available to authorized users.
Keywords
Saddle noseAugmentation rhinoplastyCartilage graftDiced cartilage in fasciaDC-FAllogenic fascia lataDeep temporalis fasciaFree diced cartilageFDC7.1 Surgical Principles in Primary Saddle-Nose Deformity
Although saddle-nose deformities are present in approximately 20 % of all rhinoplasties, the extent of saddle collapse varies widely. Hence, a wide variety of techniques are necessary to correct saddle noses. Because all saddle-nose defects arise from skeletal deficiency, augmentation is the primary means of surgical treatment. We prefer to use autologous augmentation materials for this purpose, with one exception: Tutogen (allogenic) fascia lata (Tutoplast® Inc., Neunkirchen am Brand, Germany). Tutoplast fascia lata is a gamma radiation processed human allograft which we have used successfully in over 3000 patients during the past 8 years (Fig. 7.1). Soaking the graft in antibiotic solution is necessary to rehydrate the graft and reduce infection risk. In addition to the avoidance of a donor site scar, fascia lata offers an ideal structure and stiffness for use in augmentation rhinoplasty. Conversely, autologous fascia lata lacks adequate stiffness, necessitating the use of percutaneous stay sutures to guide graft positioning and to prevent graft displacement.
As an alternative to allogenic fascia lata, we also use autologous temporalis fascia for dorsal augmentation (Fig. 7.2). However, autologous temporalis fascia has different biomechanical properties when compared to Tutoplast fascia lata. Since temporalis fascia is much thinner, the camouflage effect is reduced, and the comparative lack of graft stiffness necessitates the use of stay sutures or subcutaneous fixation sutures to maintain proper positioning. When used for radix augmentation, temporalis fascia can be compressed and suture sculpted to achieve the desired shape, and when placed over the nasion, the thick overlying skin of the radix serves to conceal irregularities in graft contour. In addition to soft-tissue augmentation, we also commonly perform dorsal augmentation using autologous cartilage harvested from a variety of donor sources including the tragus (Fig. 7.3), concha (Fig. 7.4), septum (Fig. 7.5), and rib (Fig. 7.6).
For some time, we have been using free diced cartilage (FDC) not only for dorsal refinements but also for augmentation, specifically if there is a minor contour deficiency. Cartilage harvested from the ear or rib—we avoid septal cartilage since its unique properties make it better suited to other purposes—is diced finely until it has a paste-like consistency and can be placed through the tip of a tuberculin syringe. The primary advantage of this material is its excellent malleability and reliable durability (Fig. 7.7).
We do not feel that autologous bone has a role in dorsal augmentation, and we have no clinical experience with bone grafting.
Prior to surgery, it must be decided if a full-length dorsal augmentation is preferable to a focal dorsal augmentation. Because a full-length augmentation avoids visible separations between the dorsum and the adjacent graft material, we often prefer to resect portions of the dorsum in order to facilitate a full-length (and thus far more uniform) dorsal restoration. Full-length grafts have the added advantage of creating more uniform and natural-appearing brow-tip aesthetic lines.
Although full-length augmentation is often preferable for comparatively large defects of the nasal dorsum, minor saddle indentations involving only a small portion of the dorsum are best managed with small precision-fabricated grafts custom-tailored to the defect. For this purpose, we prefer Tutoplast fascia lata, cephalic portions of the lower lateral cartilage (Fig. 7.8), tragal cartilage grafts (Fig. 7.3), or septal cartilage (Fig. 7.9) when available. Tragal cartilage is a particularly well-suited graft material for small-sized defects since we can easily harvest a 12–16-mm-wide, flat, and uniformly thick cartilage specimen with minimal donor site morbidity. When harvesting tragal cartilage, we also routinely leave behind a small outer rim of cartilage to preserve the tragal contour. Tutoplast allogenic fascia lata is available in large quantities and is well suited to virtually any sized defect. It can also be used as a single layer or as multiple layers. We have previously used as many as six layers of Tutoplast with good results, and Tutoplast can also be used to camouflage irregularities in underlying autologous cartilage grafts. Another effective method for focal dorsal augmentation is the excised cephalic remnants of the lower lateral cartilages or free diced cartilage. Noses with overly wide and bulky nasal tips often provide adequate amounts of suitable augmentation material following the cephalic trim procedure (Fig. 7.8). Morselized septal cartilage is another potential source of augmentation material (Fig. 7.9). However, the limited supply of septal cartilage must often be prioritized for other needs, and care must be taken to avoid crushing septal cartilage since unwanted chondrogenesis and/or chondrocyte mortality may lead to unacceptable long-term results.
If the saddle-nose deformity requires significantly more volume, a larger graft is required, and we often use conchal cartilage for these defects. In order to adapt the conchal graft to the appropriate shape, we incise the concave conchal surface in a grid-like pattern, leaving the outer perichondrium intact to maintain graft integrity (Fig. 7.10). When required, a double-layered graft can be used for additional graft thickness. Stability of the two-layered “sandwich” graft is enhanced by suturing the grafts in a reciprocal orientation.
When even greater volume replacement is required, our workhorse technique is the diced cartilage-fascia (DC-F) graft. Originally introduced under the moniker “Turkish delight” by Erol Onur, oxidized cellulose polymer was initially used to envelop the diced cartilage, but long-term results suffered from substantial cartilage resorption. However, the modified technique introduced by Rollin K. Daniel, which uses temporalis fascia to encase finely diced cubes of autologous cartilage measuring no more than 0.2–0.4 mm3, has virtually eliminated the problem of cartilage resorption. In order to create a uniform fascial sleeve, we use a tuberculin syringe with its tip amputated to serve as an assembly scaffold. The fascia is first wrapped around the syringe and temporarily held in position with short hub needles (Fig. 7.11). Once secured, the fascia is trimmed and sewn lengthwise to create a single longitudinal seam. After sewing the distal (cephalic) end of the sleeve shut, the syringe is then loaded with the desired amount of diced cartilage, and the cartilage is injected into the fascial sleeve (Fig. 7.12). After placement of the assembled DC-F graft into the subcutaneous pocket, we close the (open rhinoplasty) transcolumellar incision before assessing the final nasal contour. To facilitate adjustments in graft size, the proximal end of the sleeve is left open so that excess cartilage can be “milked” from the graft and removed via the marginal incision as needed. We have observed equivalent long-term results using both autologous temporalis fascia and allogenic fascia lata for sleeve construction, and diced cartilage can be constructed from septal, conchal, and rib cartilage (or combinations therein) with equal reliability.
In patients with severe dorsal defects, the solitary use of malleable augmentation materials is ill-advised since a structurally sound skeletal framework is missing. In these cases, a structural framework of solid costal cartilage must first be created to provide the necessary foundation for surface contour grafting (Fig. 7.13). Because solid rib cartilage grafts are notoriously prone to warping, special precautions must be taken when using rib cartilage. Perhaps the most important precaution is the concept of “balanced carving,” in which the graft is symmetrically harvested from the central core of the costal cartilage. In this manner the intrinsic stresses of the inner and outer cartilage components are balanced. Next, the graft is submerged in saline for a long as possible to identify any intrinsic warping tendencies not addressed by concentric carving. When identified prior to placement, warped grafts can sometimes be carved asymmetrically to balance out asymmetric stresses. Although some surgeons use a Kirschner wire to skewer the graft longitudinally for added support, we have no experience with this technique. Instead, we prefer a thick, and therefore strong, segment of solid rib cartilage, coupled with a DC-F overlay graft, for total dorsal reconstruction. As an alternative to the solid rib graft, for a while we have been using cartilaginous beam grafts consisting of two or three layers of 2–3-mm-thick stripes from rib cartilage fixed against each other.
Further stabilization is first achieved by attaching a columellar strut graft using the tongue-in-groove configuration for secure unification (Fig. 7.13). If a straight segment of rib cartilage is unavailable, the columellar strut can also be fashioned from a double-layered conchal cartilage graft.

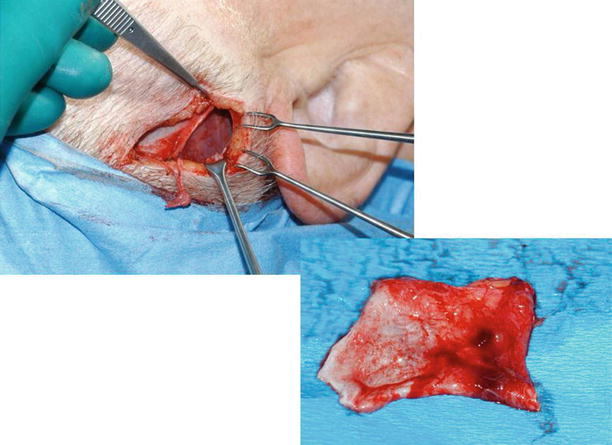
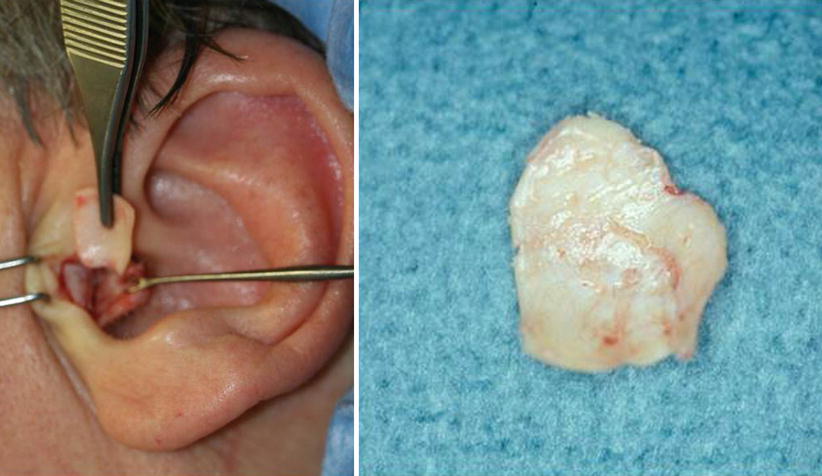

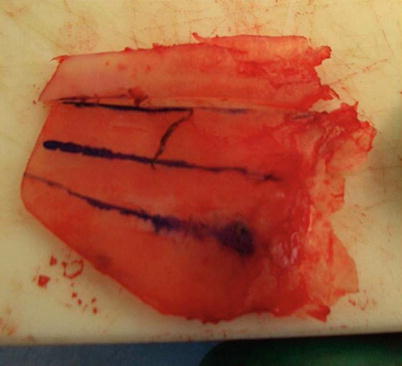

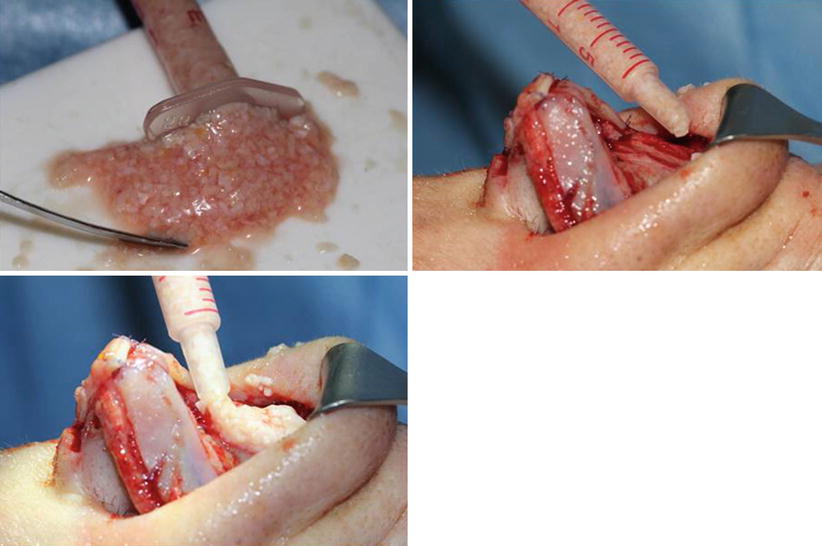
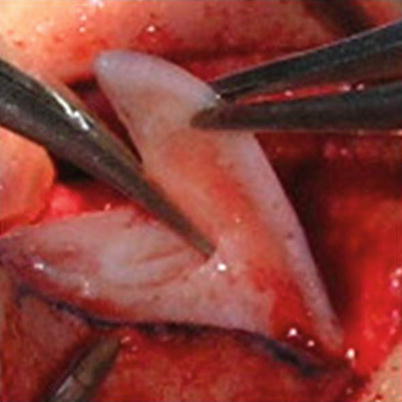
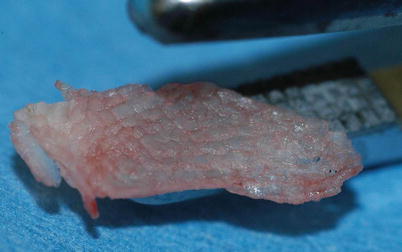




Fig. 7.1
(a) Allogenic fascia lata after rehydration. (b) Histology of explanted graft 12 months after initial placement. (c) Histology of explanted graft 14 months after initial placement
Fig. 7.2
Autologous temporalis fascia
Fig. 7.3
Tragal cartilage
Fig. 7.4
Conchal cartilage
Fig. 7.5
Septal cartilage
Fig. 7.6
Solid rib cartilage
Fig. 7.7
Finely diced cartilage for using as free graft (FDC)
Fig. 7.8
Cephalic portion of the lower lateral cartilages for augmentation
Fig. 7.9
Morselized septal cartilage
Fig. 7.10
Flattened conchal cartilage graft after cross hatching
Fig. 7.11
Tuberculin syringe with autogenous temporalis fascia attached
Fig. 7.12
DC-F with allogenic fascia lata
Fig. 7.13
Two-part solid rib cartilage graft consisting of dorsal replacement graft and integrated columellar strut graft
7.2 Case Studies
7.2.1 Case 1: Augmentation with Cephalic Portion of LLC
A 21-year-old male presented for cosmetic rhinoplasty complaining of a large nasal tip and a weak nasal dorsum. Examination revealed a wide and bulky nasal tip, thick nasal skin, and a low nasal dorsum. Treatment included resection of the LLC cephalic margin via a closed rhinoplasty approach. Tip contour was further enhanced with vertical dome division and contouring sutures. The resected portions of the LLC were then used for dorsal augmentation (Fig. 7.14).