Although office-based anesthesia for facial cosmetic surgery remains remarkably safe, no anesthesia or sedation performed outside the operating room should be considered minor. Proper organization, preparation, and patient selection, close collaboration with the surgeon, and expert and effective anesthesia care will increase patient safety and improve perioperative outcomes and patient satisfaction. This article presents a comprehensive overview of anesthesia in terms of facial plastic surgery procedures, beginning with a broad review of essentials and pitfalls of anesthesia, followed by details of specific anesthetic agents, their administration, mechanism of action, and complications.
Key points
- •
The essential anesthesia requirements for facial cosmetic surgery include a quiet, clear surgical field, absence of patient movement, nonstimulating emergence from anesthesia, a rapid return of consciousness and protective airway reflexes, prevention of postoperative nausea and vomiting, and fast-tracking patients for discharge.
- •
Facial cosmetic surgical procedures performed under sedation (monitored anesthesia care [MAC]) require extra vigilance and close cooperation between the surgeon and the anesthesiologist. Respiratory depression and rapidly ensuing upper airway obstruction caused by either absolute or relative overdose of sedative or opioid drugs can occur at any time, and may be missed if monitoring is inadequate. Patients with obstructive sleep apnea (OSA) are particularly prone to these life-threatening upper airway-related complications.
- •
Outpatient anesthesia practice is typically repetitive and predictable, and is therefore uniquely suited to protocol-driven practice improvement.
- •
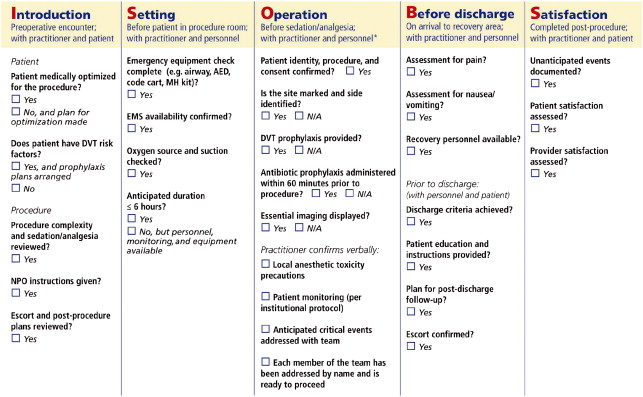
Comprehensive surgical safety checklists constitute an essential safeguard, drastically decreasing the number of perioperative complications, reducing health care costs, and improving overall quality of patient care, even when the baseline standard of care is high.
General considerations
The volume of cosmetic surgery in the United States continues to grow rapidly: more than 1.6 million surgeries were performed in 2011 alone, an increase of almost 75% since 1997. More than 80% of cosmetic surgeries are performed on the outpatient basis, and 60% in office facilities, typically demonstrating very low rates of perioperative mortality and complications, not exceeding 0.002% and 0.7%, respectively. Despite such an excellent safety profile, data from Coldiron and colleagues’ 3-year prospective audit of office-based surgical incidents in Florida suggest that facial cosmetic surgery patients may be at a higher anesthetic risk: all (albeit rare) deaths in these patients were anesthesia related, and as much as half of all major anesthetic complications (cardiovascular instability, hypoxia, respiratory failure, and so forth) were observed in this patient category. Analysis of the 2011 American Society for Aesthetic Plastic Surgery National Data Bank Statistics conservatively places the number of facial cosmetic surgical and nonsurgical procedures (eg, face lift, rhinoplasty, blepharoplasty, skin resurfacing and rejuvenation) that would require general anesthesia or various degrees of intraoperative sedation at more than 600,000 annually, thus defining the population at risk.
Structural Recommendations and Guidelines
Reducing perioperative risk and the incidence of complications in office-based cosmetic surgery is a multifaceted task ( Box 1 ), and starts with the top-down approach that introduces certain structural recommendations and guidelines. The anesthesiologist (and the surgeon) should follow the provisions of the American Society of Anesthesiologists (ASA) Guidelines for Ambulatory Anesthesia and Surgery, the ASA Guidelines for Office-Based Surgery, the ASA Standards for Basic Anesthetic Monitoring, and the ASA Standards for Postanesthesia Care, to ensure that the quality of patient care will meet hospital-based standards.
- •
Accredited surgical facility
- •
Top-down approach to assure compliance with American Society of Anesthesiologists guidelines and presence of established policies and procedures
- •
Bottom-up approach with quality improvement and personnel training
- •
Presence of expert anesthesiologist and surgeon with appropriate knowledge and experience in office-based surgery
- •
A team approach to patient care
- •
Safety checklists
Some of the essential requirements for patient safety in the office-based surgical setting are :
- •
Accreditation of the facility by either the American Association for Accreditation of Ambulatory Surgical Facilities, the Accreditation Association for Ambulatory Health Care, or the Joint Commission
- •
Proper patient and procedure selection
- •
Availability of essential anesthesia and resuscitative equipment, including malignant hyperthermia cart and difficult airway equipment
- •
Existence of emergency protocols and patient transfer agreements
- •
Education and training of office personnel
Solutions to Identified Problems
It is equally important for the surgeon and anesthesiologist to have an effective bottom-up approach to office-based patient care, ensuring proper documentation and analysis of complications and adverse events, and the development of solutions to the identified problems. Outpatient anesthesia practice is typically repetitive and predictable, and is therefore uniquely suited to protocol-driven practice improvement.
Surgical Safety Checklists
Comprehensive surgical safety checklists constitute another safeguard, drastically decreasing the number of perioperative complications, reducing health care costs, and improving overall quality of patient care, even when the baseline standard of care is high. For office-based surgery, implementation of a checklist developed by the Institute for Safety in Office-Based Surgery ( Fig. 1 ) has resulted in a 6-fold decrease in the incidence of perioperative complications.
General considerations
The volume of cosmetic surgery in the United States continues to grow rapidly: more than 1.6 million surgeries were performed in 2011 alone, an increase of almost 75% since 1997. More than 80% of cosmetic surgeries are performed on the outpatient basis, and 60% in office facilities, typically demonstrating very low rates of perioperative mortality and complications, not exceeding 0.002% and 0.7%, respectively. Despite such an excellent safety profile, data from Coldiron and colleagues’ 3-year prospective audit of office-based surgical incidents in Florida suggest that facial cosmetic surgery patients may be at a higher anesthetic risk: all (albeit rare) deaths in these patients were anesthesia related, and as much as half of all major anesthetic complications (cardiovascular instability, hypoxia, respiratory failure, and so forth) were observed in this patient category. Analysis of the 2011 American Society for Aesthetic Plastic Surgery National Data Bank Statistics conservatively places the number of facial cosmetic surgical and nonsurgical procedures (eg, face lift, rhinoplasty, blepharoplasty, skin resurfacing and rejuvenation) that would require general anesthesia or various degrees of intraoperative sedation at more than 600,000 annually, thus defining the population at risk.
Structural Recommendations and Guidelines
Reducing perioperative risk and the incidence of complications in office-based cosmetic surgery is a multifaceted task ( Box 1 ), and starts with the top-down approach that introduces certain structural recommendations and guidelines. The anesthesiologist (and the surgeon) should follow the provisions of the American Society of Anesthesiologists (ASA) Guidelines for Ambulatory Anesthesia and Surgery, the ASA Guidelines for Office-Based Surgery, the ASA Standards for Basic Anesthetic Monitoring, and the ASA Standards for Postanesthesia Care, to ensure that the quality of patient care will meet hospital-based standards.
- •
Accredited surgical facility
- •
Top-down approach to assure compliance with American Society of Anesthesiologists guidelines and presence of established policies and procedures
- •
Bottom-up approach with quality improvement and personnel training
- •
Presence of expert anesthesiologist and surgeon with appropriate knowledge and experience in office-based surgery
- •
A team approach to patient care
- •
Safety checklists
Some of the essential requirements for patient safety in the office-based surgical setting are :
- •
Accreditation of the facility by either the American Association for Accreditation of Ambulatory Surgical Facilities, the Accreditation Association for Ambulatory Health Care, or the Joint Commission
- •
Proper patient and procedure selection
- •
Availability of essential anesthesia and resuscitative equipment, including malignant hyperthermia cart and difficult airway equipment
- •
Existence of emergency protocols and patient transfer agreements
- •
Education and training of office personnel
Solutions to Identified Problems
It is equally important for the surgeon and anesthesiologist to have an effective bottom-up approach to office-based patient care, ensuring proper documentation and analysis of complications and adverse events, and the development of solutions to the identified problems. Outpatient anesthesia practice is typically repetitive and predictable, and is therefore uniquely suited to protocol-driven practice improvement.
Surgical Safety Checklists
Comprehensive surgical safety checklists constitute another safeguard, drastically decreasing the number of perioperative complications, reducing health care costs, and improving overall quality of patient care, even when the baseline standard of care is high. For office-based surgery, implementation of a checklist developed by the Institute for Safety in Office-Based Surgery ( Fig. 1 ) has resulted in a 6-fold decrease in the incidence of perioperative complications.
Perioperative and anesthetic management
Anesthetic management of patients undergoing facial cosmetic surgery presents unique challenges to the anesthesiologist. The absent or limited anesthesia backup, inadequate ancillary support, lack of anesthesia equipment, variability of monitoring modalities, and cramped and unfamiliar environment may all make the delivery of anesthesia care in the office-based setting difficult.
To provide safe and effective anesthesia care, the anesthesiologist should be experienced with the office-based surgery, serve as a competent consultant for proper patient selection and preparation, understand anesthesia objectives for facial cosmetic surgical procedures, be well versed with total intravenous anesthesia (TIVA) and administering effective sedation without immediate access to the patient’s airway, and possess some of the unique techniques of advanced airway management.
Anesthesia Objectives
The essential anesthesia requirements for facial cosmetic surgery include a quiet, clear surgical field, absence of patient movement, nonstimulating emergence from anesthesia, a rapid return of consciousness and protective airway reflexes, prevention of postoperative nausea and vomiting (PONV), and fast-tracking patients for discharge.
Maintenance of a clear surgical field is extremely important owing to the high vascularity of the operated areas, where even a small amount of bleeding can have a significant impact on intraoperative exposure. The use of moderate controlled hypotension by the anesthesiologist (see later discussion), and epinephrine-supplemented infiltrative local anesthesia by the surgeon improve both hemostasis and visibility.
Absence of patient movement is required for preventing iatrogenic surgical injury during the delicate parts of the procedure. If general anesthesia is used, deeper anesthetic planes may be necessary to avoid sudden patient motor responses, as intraoperative neuromuscular blockade (NMB) is usually avoided. It is also important for the anesthesiologist to maintain situational awareness in the crowded operating room (OR) environment, to avoid any inadvertent action that may result in accidental movement of the OR table.
Smooth emergence from anesthesia, devoid of patient straining, bucking, and coughing, is essential for avoiding the formation of hematoma, which may require surgical drainage or reexploration, especially after rhytidectomy. Avoidance of PONV is equally important in this regard, and will also reduce the recovery time and the incidence of unanticipated hospital admissions.
Assuring a rapid emergence and return of consciousness as well as protective airway reflexes is critical, as supporting the patient’s airway with mask ventilation after facial cosmetic surgery will either be difficult (eg, rhytidectomy) or impossible without jeopardizing the cosmetic surgical results (eg, rhinoplasty).
Provision of anesthesia care aimed at fast-tracking patients for discharge is dictated by the overwhelmingly outpatient nature of the facial cosmetic surgical procedures, and by economic considerations of office-based surgery.
A high degree of cooperation with the surgeon is essential to ensure consensus regarding anesthesia objectives, other unique perioperative considerations for a specific procedure, and expectations about patient comfort and satisfaction.
Patient Selection and Preparation
Preoperative risk assessment should take into account the type of facial cosmetic surgery to be performed, and the patient’s health status. Most patients presenting for facial cosmetic surgery are either completely healthy (ASA physical status I) or have a mild, controlled systemic disease (ASA physical status II). However, a variety of even “stable” comorbidities may affect surgical outcomes and perioperative management of these patients.
Special attention should be directed to conditions such as preexisting cardiovascular disease, particularly systemic hypertension (HTN), which may predispose the patients to hematoma formation. Preoperatively, HTN should be well controlled, and it may be prudent to either decrease the concentration of epinephrine in local anesthetic mixture, or to avoid epinephrine completely in selected patients. Evaluation of the patient’s cardiac status should follow the American College of Cardiology and American Heart Association guidelines on perioperative evaluation and care for noncardiac surgery. If patient’s baseline functional capacity is moderate to excellent, no additional cardiac testing is required: facial cosmetic surgical procedures carry a low (<1%) risk of major cardiac complications, such as cardiac death or nonfatal myocardial infarction. Preoperative and postoperative resting 12-lead electrocardiograms are not indicated in asymptomatic patients undergoing low-risk surgical procedures. Likewise, routine preoperative laboratory testing before elective, low-risk ambulatory surgery is not indicated.
Pulmonary status of patients with chronic obstructive pulmonary disease should be carefully evaluated and optimized to decrease the possibility of postoperative pulmonary complications. Cigarette smoking is associated with a 12- to 20-fold increase in risk of flap slough, and abnormal airway reactivity may provoke excessive postoperative coughing and straining, increasing the risk of postoperative bleeding. Chronic cigarette smoking and alcohol use also cause an induction of the cytochrome P450 multienzyme system, leading to increased perioperative requirements for opioids and neuromuscular blockers, and generation of higher levels of potentially toxic metabolites of halogenated volatile anesthetic agents.
Patients with diabetes mellitus and those with rheumatologic diseases may be particularly prone to bruising, infection, and delayed healing. The use of nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin, herbal supplements such as Gingko, Echinacea, and St John’s wort, and certain vitamins (eg, vitamin E) should be stopped at least 2 weeks before surgery, to avoid the risk of excessive microvascular bleeding.
Healthy elderly patients can undergo office-based anesthesia safely, but the anesthesiologist should be aware of pathophysiologic implications of advanced age on organ function and pharmacokinetics of anesthetic drugs. Elderly patients will require careful attention to positioning and the maintenance of intraoperative normothermia.
The patients with obesity and those with the history of difficult airway should be approached with particular caution, and the anesthesiologist should be consulted early. Patients with obstructive sleep apnea (OSA) should be carefully screened for suitability for same-day facial cosmetic surgery. Sleep-disordered breathing is extremely common, affecting nearly 20% of the adult population, with 7% to 8% suffering from moderate to severe OSA. It is estimated that more than 20% of the adult surgical population suffer from OSA, which remains undiagnosed in the majority (70%) of patients. When screening for the presence of OSA during a preoperative office visit, a physician may wish to use the highly sensitive and validated STOP-BANG questionnaire ( Table 1 ).
| S nore loudly? | B ody mass index >35 kg/m 2 ? |
| T ired during the day? | A ge >50 y? |
| O bserved cessation of breathing during sleep? | N eck circumference >40 cm? |
| P ressure (high blood pressure)? | G ender male? |
OSA adversely affects a variety of organ systems, with widespread implications for the surgical patient. The presence and severity of OSA is strongly correlated with obesity and metabolic syndrome, systemic and pulmonary HTN, congestive heart failure, arrhythmias, heart attacks, and stroke. Patients with either known or presumed OSA should undergo outpatient surgery only if their comorbidities are optimized, if postoperative pain is going to be mild and can be predominantly managed with nonopioid analgesics, and if (for continuous positive airway pressure [CPAP] users) the patients can continue to use CPAP postoperatively. For practical purposes, patients with severe OSA (ASA physical status III) should not routinely undergo office-based surgery under general anesthesia or sedation.
Intraoperatively, OSA patients demonstrate enhanced sensitivity to opioids and benzodiazepines, which may lead to rapidly developing respiratory depression, upper airway collapse, and airway obstruction. Conscious sedation of these patients, as well as those with obesity, should be performed with extreme caution. The OSA patients may also present with difficult airway problems, related to both difficult mask ventilation and tracheal intubation.
A multimodal approach that minimizes narcotic medications (eg, NSAIDs, acetaminophen, cyclooxygenase-2–specific inhibitors) should be used perioperatively whenever feasible. Postoperatively, the ASA recommends to extend monitoring of the OSA patients for an additional 3 hours. It is best to schedule these patients earlier in the day to facilitate this, and transfer procedures to an inpatient facility should be in place should complications arise.
Patients’ status should nothing by mouth on the day of surgery in accordance with the ASA Guidelines for Preoperative Fasting. Clear fluid intake can be allowed for up to 2 hours before the start of surgery in otherwise healthy patients presenting for elective procedures.
Premedication and Monitoring
Standard premedication with intravenous short-acting benzodiazepine (eg, midazolam) is used routinely. Antibiotic prophylaxis (eg, intravenous cefazolin) is typically administered in the majority of cases. Routine ASA monitoring is usually sufficient, even if controlled hypotension is used intraoperatively.
Patient Positioning and Prophylaxis of Thromboembolism
Ulnar neuropathies and brachial plexus injuries are most prevalent among perioperative nerve injuries, can also be observed under monitored anesthesia care (MAC), but are extremely rare in cosmetic surgery. Hoefflin and colleagues recorded only 1 case of peripheral neuropathy in more than 23,000 general anesthetics, perhaps reflecting the absence of risk factors for nerve damage in a healthy patient population and meticulous attention to patient positioning during office-based surgery.
Padded support (eg, lumbar area, neck) for the patient is best provided before induction of anesthesia to assure a comfortable position for the patient on the OR table for the duration of surgery, and the patient’s arms and all the pressure points must be well protected intraoperatively. For MAC cases, assuring the utmost comfort of the patient on the OR table before the start of surgery will also greatly facilitate provision of anesthesia care and the patient’s tolerance of long procedures. The use of forced-air warming, particularly during general anesthesia and in the elderly, facilitates maintenance of intraoperative normothermia. The patient’s eyes are usually protected in the field by the surgeon.
Free access to the patient’s airway is usually difficult or impossible, as the OR table is turned 90° or 180° away from the anesthesiologist. If general anesthesia is used, the anesthesiologist must thoroughly check the anesthesia circuit connections to prevent accidental disconnect under the surgical drapes, and the dedicated artificial airway must be diligently taped.
The use of the lower extremity sequential compression devices (SCDs) for prophylaxis of deep venous thrombosis (DVT) and intraoperative pulmonary embolism (PE) in anesthetized patients has become routine, and should be instituted before the induction of general anesthesia.
Anesthetic Management
A wide variety of office-based cosmetic procedures can be safely and effectively performed under either local anesthesia with intravenous sedation (MAC) or general anesthesia. The choice is frequently dictated by the patient’s desires and the surgeon’s level of comfort.
Death (26%), nerve damage (22%), permanent brain damage (9%), airway injury (7%), and medication errors (7%) represent some of the most common major anesthesia-related complications, according to the ASA Closed Claims Project database containing 8954 anesthesia malpractice claims. Adverse respiratory and cardiovascular incidents accounted for 17% and 13% of all claims associated with anesthesia-related sentinel events. Among the respiratory incidents, difficult intubation, inadequate oxygenation or ventilation, and pulmonary aspiration were the most common, and by proxy may be expected to account for the majority of patient morbidity during office-based anesthesia. In particular, inadequate oxygenation/ventilation has become a growing problem during MAC cases and administration of anesthesia in the non-OR environment. Moreover, between 1997 and 2007 more than 40% of malpractice claims associated with MAC involved the patient’s death or permanent brain damage.
Cardiovascular incidents are not expected to be prevalent in office-based cosmetic surgery. Most cardiovascular events leading to anesthesia claims between 1990 and 2007 were related to hemorrhage/blood replacement, fluid management/electrolyte abnormalities, and stroke. No major cardiovascular morbidity associated with general anesthesia was observed by Hoefflin and colleagues in more than 23,000 patients who had undergone cosmetic and facial cosmetic surgery in the office-based setting.
Medication problems are relatively common, and represented 7% of anesthesia claims between 1990 and 2007. These claims were fairly equally distributed between adverse drug reactions and medication errors, and most medication errors were considered preventable.
Most anesthesia-related complications in ambulatory surgery are expected to be minor, with the commonly cited incidence of :
- •
PONV 4.7%
- •
Shivering 2.2%
- •
Eye injury 0.056%
- •
Dental injury 0.02%
- •
Ulnar neuropathy 0.47%
- •
Sore throat 28%
Conscious sedation
Eliminating the need for general anesthesia avoids invasive airway management, removes the triggers for malignant hyperthermia and emergence phenomena, reduces the incidence of PONV, and facilitates patient discharge.
The authors’ experience corroborates that of others that administering a successful MAC without immediate access to the patient’s airway is frequently more challenging than conducting the general anesthesia. Safe management of fluctuating levels of noxious stimulation, appreciation of pharmacokinetic profile and additive and synergistic effects of administered intravenous drugs, and variability of patient responses require a high level of vigilance and skill.
Respiratory depression resulting from either absolute or relative overdose of sedative or opioid drugs can occur at any time, and was the leading (21%) mechanism associated with inadequate oxygenation/ventilation and death/permanent brain damage in MAC malpractice claims. Nearly half of these claims were judged as preventable by :
- 1.
Better monitoring, including capnography
- 2.
Improved vigilance
- 3.
Presence of audible monitoring alarms
MAC claims in facial cosmetic and plastic surgery are relatively common, accounting for more than 25% of all MAC claims between 1997 and 2007. In the audit by Coldiron and colleagues, all facial cosmetic surgical deaths were MAC related. This finding is not surprising, because during the facial procedures the visibility of the patient’s airway is impaired, and capnography monitoring may become unreliable. The use of the precordial stethoscope placed over the patient’s trachea to monitor breath sounds can be advantageous in such cases.
Intraoperatively, the patient care team should appreciate that MAC represents a continuum of the sedation states, which can quickly progress from a moderate level (“conscious sedation”) to deeper planes whereby spontaneous ventilation may be inadequate, and further to general anesthesia, whereby a patient becomes unresponsive and airway support will be frequently required. Every planned MAC should be treated as a potential case of general anesthesia. When intravenous sedation is administered by nonanesthesiologist, at least one individual capable of establishing a patent airway and instituting positive pressure ventilation should be continually present throughout the procedure.
Conducting safe and successful MAC requires the anesthesiologist to appreciate pharmacokinetic and pharmacodynamic interactions of the chosen intravenous sedating agents, as well as the role of pharmacologic antagonists for opioids and benzodiazepines. A synergistic effect of the sedating agents should be kept in mind to avoid rapid onset of respiratory depression and upper airway obstruction, and the doses of the administered medications should be appropriately reduced. The desired level(s) of sedation should be clearly defined and discussed with the surgeon preoperatively. Once these objectives are established, the choice, and the safe and rational use of intravenous sedating and hypnotic agents will largely depend on the preference and experience of the anesthesiologist.
Intravenous opioids
Discussed here are:
- •
- •
- •
- •
- •
- •
Intravenous opioids, especially those with rapid onset (alfentanil, remifentanil), may be particularly useful, as they provide intense analgesia of short duration, have a sedative effect, and possess excellent antitussive properties. One may expect almost identical peak effect time of an equipotent single bolus dose of remifentanil and alfentanil (0.9 minutes and 1.3 minutes, respectively), whereas significant delay is observed for fentanyl (3.3 minutes) and sufentanil (8.5 minutes). The analgesic effect of a single bolus dose of remifentanil is 20 to 30 times higher than that of alfentanil.
Remifentanil
Remifentanil can be given as a bolus dose of 1 to 2 μg/kg, which is usually well tolerated by awake patients, and can also be administered by infusion, which will facilitate hemodynamic stability and reduce the incidence of opioid-induced side effects. Continuous infusions of remifentanil, 0.05 to 0.08 μg/kg/min, projected to reach a steady-state concentration of 1.3 to 2 ng/mL in 30 to 40 minutes, seem to be well tolerated by awake patients. The anesthesiologist must keep in mind that remifentanil blood concentrations of 1.3 to 2 ng/mL are substantial, and correlate with those required to reduce minimum alveolar concentration of isoflurane by 50% and block sympathetic responses to skin incision in 50% of patients (EC 50 ) receiving target-controlled propofol anesthetic, respectively.
A higher sensitivity to, and slower onset of remifentanil in the elderly should be expected, as these patients also tend to have a smaller volume of distribution and lower remifentanil clearance. The initial loading dose of remifentanil in patients older than age 65 years should be decreased by 50% and then adjusted as required, according to the individual patient’s response.
Alfentanil
In contrast to remifentanil, the pharmacodynamic effects of alfentanil are more variable, with the corresponding range of adequate plasma analgesic concentrations (20–60 ng/mL) for many of the awake, but sedated patients. This concentration falls within that for adequate ventilation (EC 50 45–60 ng/mL) as well. Based on the available pharmacokinetic modeling data, a 60-ng/mL target concentration of alfentanil can probably be achieved in the majority of patients with a single alfentanil bolus dose 7 to 10 μg/kg.
Midozolam
The opioids alone fail to provide sufficient levels of sedation and amnesia, and their combination with intravenous benzodiazepines is usually highly desirable. Midazolam is widely used for procedural sedation, owing to its potent anxiolytic and amnestic properties, rapid effect-site equilibration, good titratability, and relatively short half-life. However, substantial pharmacodynamic variability with regard to amnestic effect exists between the patients, and coadministration of midazolam with opioids may quickly result in oversedation, hypoventilation, apnea, or airway obstruction. If a midazolam-remifentanil combination is used, lower doses of midazolam (1–2 mg) may be advisable and careful titration is paramount. In the absence of well-defined points of titration (eg, Ramsay Sedation Scale of 2–3), administration of midazolam may result in several undesirable outcomes, such as the need for respiratory intervention that may disrupt surgery (eg, the need for airway support), slower recovery, recall despite attempted amnesia, and a risk of “atypical” reaction characterized by patient agitation necessitating a conversion to general anesthesia.
Propofol
Similar considerations apply to a combination of intravenous opioids with propofol. Propofol offers certain advantages over benzodiazepines, including faster onset, rapid awakening, and ease of titration. The combination of opioids with propofol produces a full synergistic effect, with each drug increasing each other’s sedative and analgesic properties, and this synergy is more pronounced for remifentanil than for other opioids. A combination with an opioid should be expected to increase the risk of significant respiratory depression, as both the ventilatory responses to hypercapnia and hypoxemia are diminished during propofol administration. If such a combination is desired, it is advisable to target an effect-site concentration lower than optimal for opioids and higher than optimal for propofol, to preserve adequate spontaneous ventilation.
Dexmedetomidine
Respiratory depression presents few issues if dexmedetomidine, a highly selective, centrally acting α2-adrenoreceptor agonist, is used for MAC. Dexmedetomidine produces anxiolysis and sedation in a dose-dependent fashion, potentiates opioid analgesia, possesses antisialagogue, antitussive, and sympatholytic properties, and causes only minimal, if any, respiratory depression. Thus dexmedetomidine has low likelihood for airway intervention, may decrease or eliminate supplemental oxygen requirements during laser facial cosmetic procedures, and improves patient cooperation. In a retrospective study by Taghinia and colleagues the use of dexmedetomidine during MAC or general anesthesia in patients undergoing face lift (rhytidectomy) resulted in reduced use of midazolam, fentanyl, and propofol, produced fewer episodes of intraoperative hypoxemia, and facilitated maintenance of intraoperative hypotension; in addition, the incidence of PONV was also reduced.
Dexmedetomidine demonstrates delayed onset of action of approximately 15 minutes, and peak concentrations are usually achieved within 1 hour following continuous intravenous infusion, which make the drug poorly titratable. Nevertheless, its stable and predictable pharmacokinetic profile makes it relatively easy to administer. A typical loading dose is 0.5 to 1.0 μg/kg bolus over 10 minutes, followed by a continuous infusion of 0.2 to 1.0 μg/kg/h, titrated to a Ramsay sedation score of 2 or greater, has been advocated. It should be noted that the bolus doses of dexmedetomidine exceeding 1 μg/kg, especially when administered rapidly, may be associated with short periods of hypercapnia, hypoxemia, and apnea.
Despite reliably producing a state of cooperative sedation, when used alone dexmedetomidine possesses little, if any, amnestic properties, and a combination with small doses of midazolam may be desired. Analgesic properties of dexmedetomidine are also mild, and the anesthesiologist must be prepared to supplement analgesia with short-acting opioids (eg, remifentanil, alfentanil) during the most stimulating parts of the surgical procedures. Again caution is needed, as this combination may result in increased likelihood of hypoventilation, apnea, and airway compromise.
The limitations of the use of dexmedetomidine for outpatient surgery come from its pharmacokinetic profile and the mechanism of action. Delayed peak effect impairs clinical efficiency, and may also lead to prolonged stay in the recovery room. The potent sympatholytic effect of dexmedetomidine may lead to intraoperative bradycardia and hypotension, which may persist during the recovery period; bradycardia may be further enhanced by the addition of remifentanil.
Ketamine
A combination of dexmedetomidine and ketamine may be particularly beneficial. Ketamine causes sympathetic stimulation, counteracting the sympathetic depressant effects of dexmedetomidine; provides reliable and rapid amnesia; does not cause respiratory depression; and possesses analgesic properties. The antisialagogue effect of dexmedetomidine offsets the ketamine-induced hypersalivation; further decrease in secretions can be enhanced by pretreatment with glycopyrrolate, which, in turn, may also counteract dexmedetomidine-induced bradycardia. A ketamine bolus dose of 0.5 mg/kg can be recommended to induce a dissociative state of consciousness, and maintenance with a low-dose continuous infusion 3 to 10 μg/kg/min (target concentration 50–100 ng/mL) should facilitate additional analgesia and the state of a light hypnosis. Although not vigorously investigated, a combination of ketamine and propofol, popularized by Friedberg, is claimed to be highly effective, allowing avoidance of the use of intraoperative opioids.
Despite its excellent safety profile, at deeper levels of sedation ketamine can still cause airway obstruction, laryngospasm, and pulmonary aspiration, especially in combination with other sedating agents. Furthermore, because of the induced dissociative state, assessment of the degree of sedation with ketamine may be difficult: the patient’s eyes may remain open and the eye movements may be preserved even in a state of deep sedation or general anesthesia.
Successful conscious sedation
The key to success of the MAC-based facial cosmetic surgery remains adequate local and regional anesthesia performed by the surgeon. The anesthesiologist and the surgeon should be thoroughly familiar with the safe total dose of a local anesthetic that can be administered to the patient. The anesthesiologist should also be made aware of the use of the local anesthetic-epinephrine mixture by the surgeon to closely observe (and treat, where appropriate) the ensuing hemodynamic responses of the patient. These responses may be exaggerated in older patients and those with coexisting cardiovascular disease, requiring prompt treatment.
Burn injuries resulting from on-patient operating room fires, particularly during head and neck surgery, have accounted for 20 MAC malpractice claims (17%) between 1997 and 2007. All these burns were triggered by the use of electrocautery (diathermy), in the presence of supplemental oxygen administration to the patient, and the use of alcohol-containing prep solution and surgical drapes in the field. The possibility of burn injuries during facial cosmetic surgery is reduced with general anesthesia, whereby the oxygen delivery system (eg, endotracheal tube [ETT] or laryngeal mask airway [LMA]) is usually sealed to the atmosphere. The use of the ETT or LMA is recommended for MAC with moderate to deep sedation, which require oxygen supplementation, and/or in oxygen-dependent patients who undergo surgery of the head, neck, or face. The prevention and management of on-patient OR fires should follow the ASA Practice Advisory. Table 2 lists some of the most important considerations.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


