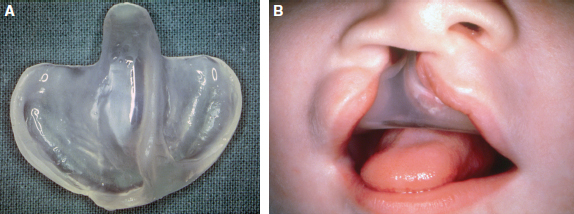
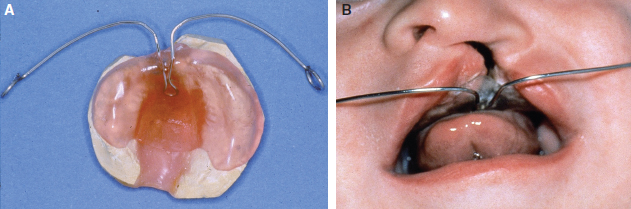
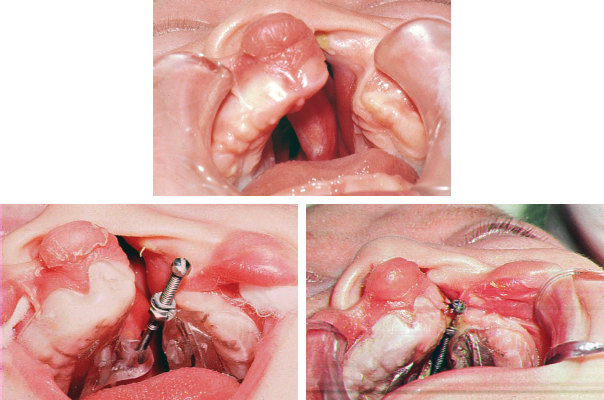
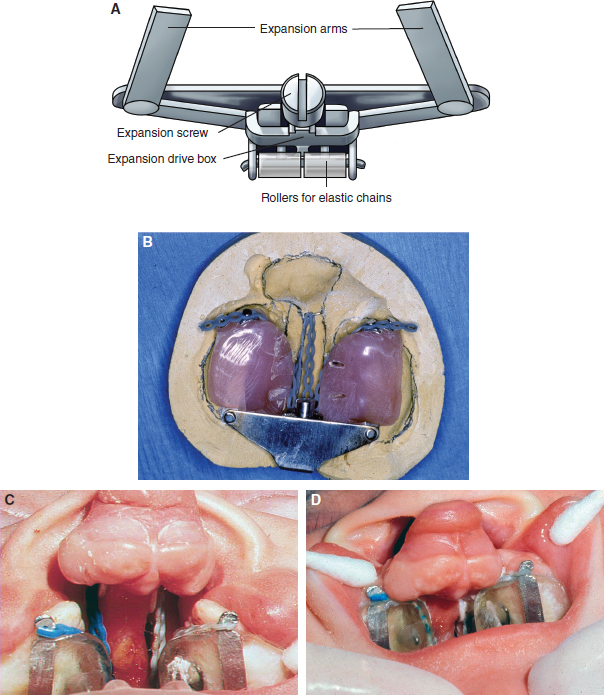
63 ○ Presurgical infant orthopedics (PSIO) is performed in an attempt to improve the lip and palate repair by realigning the displaced maxillary bony segments found in clefts. ○ Passive appliances are acrylic plates that are adjusted frequently to apply a combination of pressure on one side and relief on the other that directs the bony growth of the maxillary segments into alignment. ○ Active appliances are fixed to the bony segments with pins or screws, and the segments are aligned with jackscrews and elastic bands. ○ The addition of nasal extensions by Grayson and his colleagues led to the development of nasoalveolar molding. ○ PSIO has generally been shown to be effective in improving the alignment of the maxillary segments before lip and palate surgery. ○ Whether PSIO improves long-term outcomes of nasolabial appearance, dental alignment, and palatal function when compared with patients who do not have PSIO is a subject of considerable disagreement. C. Kerr McNeil1–3 first described presurgical infant orthopedics (PSIO) in cleft care in 1950 when he introduced the concept of using orthodontic appliances to realign the maxillary segments in infants with clefts of the lip and palate. He proposed that repositioning the maxillary segments would facilitate the surgical repair of the lip and palate and improve symmetry of the maxilla, lip, and nose. The practice of PSIO was founded in the belief that repositioning the palatal segments and dental arches will facilitate the surgical repair of the lip and palate, ease alveolar bone grafting, and simplify orthodontic treatment. Proponents felt that repositioning the premaxilla and lateral palatal shelves would prevent the maxillary retrusion commonly seen in patients with clefts. They also hypothesized that the improved maxillary alignment would also allow concurrent symmetric growth of the mandible that, in turn, would allow for a more stable correction of the dental malocclusion.4 Bilateral clefts appeared to be particularly suited to the technique. Appliances were used to reposition the premaxilla posteriorly after expanding the lateral segments, thereby facilitating the lip repair.5,6 Although the theoretical advantages of PSIO allowed the technique to gain popularity, it wasn’t until its use in conjunction with primary alveolar bone grafting that it became widely practiced.7 Despite early reports of impaired maxillary growth with primary alveolar grafting, reports of favorable outcomes existed as well.5,6,8–10 Burston,5,6 an orthodontist from England and strong proponent of early bone grafting in combination with PSIO, stated that the main objective of PSIO with primary bone grafting was to prevent palatal collapse, to maintain normal alveolar alignment, and to promote eruption of deciduous teeth with appropriate dental relationships. He also claimed these patients had improved respiration, feeding, speech, and middle-ear function, although these claims were certainly not grounded in sufficient evidence. Before the advent of PSIO, some surgeons attempted to align the facial skeleton by performing premaxillectomies, either in infancy or in later childhood. These procedures resulted in severe underdevelopment of the midface, collapse of the maxilla, failure of growth of the prolabium, and loss of support for the upper lip.11 Fortunately, this procedure has been abandoned. Many terms have been applied to techniques of presurgical maxilloalveolar molding, soft tissue manipulation, or a combination of the two. Common terms include presurgical infant orthopedics, neonatal maxillary orthopedics, and nasoalveolar molding. The design and application of these appliances have varied considerably. Notable contributions to the field have been made by Hotz,8 Latham,12 Rosenstein,13 and Grayson et al.14 Appliances can be divided into two broad categories: passive and active. Passive appliances use acrylic plates that are constructed in a manner that applies pressure to the palatal segments in the direction of the desired movement and relief on the opposite side to accommodate the moving palatal shelf. The acrylic plates require frequent adjustments by the dentist or orthodontist to continue directing palatal growth. New appliances are made as needed to accommodate the growing maxilla (Figs. 63-1 and 63-2). Fig. 63-1 A, Passive acrylic appliance. B, Appliance in place. Fig. 63-2 A, Passive appliance built on a plaster model. B, Passive appliance with extensions attached to headband. Grayson et al14 added nasal extensions to the appliance to reshape the nostrils. Presurgical nasoalveolar molding (NAM), discussed in more detail in Chapter 64, addresses the soft-tissue derangements of the lip, palate, and nose. The technique not only aligns the maxillary segments but also takes advantage of the principles of tissue expansion and the malleability of the infant nasal cartilages to reshape and align the soft tissues. Columellar length and shape is improved, especially in bilateral clefts, and lip repair is thereby made simpler. Despite the obvious advantages, the cost-effectiveness and long-term efficacy of the technique are questionable. Active appliances, popularized by Latham, are fixed intraorally with screws, elastic chains, or plates used to apply direct traction forces to align the palatal segments (Figs. 63-3 and 63-4). Fig. 63-4 An active pin–retained device with a jackscrew used to approximate the maxillary segments. Controversy surrounds the use of PSIO as much now as it did in the 1960s, at which time Pruzansky criticized the widespread acceptance of PSIO, citing that many of its proponents relied not on evidence but on anecdotal reports and uncontrolled studies. In his paper “Presurgical Orthopedics and Bone Grafting for Infants With Cleft Lip and Palate: A Dissent,”15 Pruzansky pointed out that without well-designed, controlled studies, claims that the technique facilitated lip and palate repair and improved feeding, speech, and psychological outcomes could not be substantiated. He also drew attention to the fact that proponents of the McNeil method had limited evidence to support the dominance of the nasal septum as a growth force and had failed to consider the effect that repositioning the orbicularis muscle exerts on the dynamic palatal segments. Perhaps what was most important, he contested the notion that collapse of the maxillary arch is an undesirable side effect of primary cheiloplasty. He felt that preventing medialization of the palatal shelves with interposition of a palatal splint would be detrimental to reestablishing velopharyngeal competence. Anatomic studies have demonstrated that the nasopharynx of the cleft side is wider than that of the noncleft side.16 After lip repair, medial movement of the maxillary arch narrows the cleft side nasopharynx to a more normal dimension, an effect considered desirable. More recently, Winters and Hurwitz17 concluded that the objective evidence in support of PSIO is lacking. To consider the advantages and disadvantages of PSIO, understanding the changes that occur after the lip and palate are repaired without the use of PSIO is necessary. Mazaheri and colleagues18–21 of the Lancaster Cleft Palate Clinic demonstrated the effect that primary lip closure exerts on the palate in a longitudinal analysis of patients with unilateral cleft lip and palate: • The palatal cleft narrows as the palatal segments are repositioned. • Downward growth and change in angulation of the palatal segments accounted for by the inherent medial growth of the palatal shelves occurs. • The greater and lesser palatal segments continue to undergo favorable change and repositioning with eruption of the deciduous dentition.
Presurgical Infant Orthopedics
Brett F. Michelotti, Mohammad Mazaheri, Donald R. Mackay
KEY POINTS
PASSIVE APPLIANCES
ACTIVE APPLIANCES
EFFICACY OF PRESURGICAL INFANT ORTHOPEDICS
Lip Repair Without Presurgical Infant Orthopedics
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


