Preoperative Sizing in Breast Augmentation
David A. Hidalgo, M.D.
Jason A. Spector, M.D.
New York, N.Y.
From the Division of Plastic Surgery, Weill Cornell Medical College.
Received for publication June 22, 2009; accepted September 8, 2009.
Copyright © 2010 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e3181cb6530
Disclosure: Neither of the authors has a financial interest in any of the products or devices mentioned in this article.
Background: Implant size selection in breast augmentation patients is one of many variables to be determined before surgery. Few methods exist today that allow the patient to participate in this process and accurately determine optimal size. The authors describe a simple method of preoperative sizing using silicone implant samples.
Methods: A total of 567 patients underwent breast augmentation: 297 had surgery before implementation of preoperative sizing and 270 patients were sized preoperatively. Sizing consisted of fitting the patients with various size silicone implants in a larger bra at least twice before surgery to determine desired size. Surveys were sent to both groups to inquire about overall satisfaction, how many preferred a different size postoperatively, and how many ultimately underwent size change surgery.
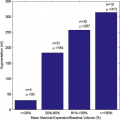
Results: One hundred two responses (34.3 percent) were obtained from the control group and 142 (52.6 percent) were obtained from the sized group. Sized patients received smaller implants (average, 276.6 cc nonsized versus 246.4 cc sized; p < 0.001). Four patients (1.4 percent) in the control group underwent a size change procedure compared with none in the sized group. In the sized cohort, 69 percent believe they are the size that the process predicted, 21 percent are smaller, 9 percent are larger, and 1 percent did not answer the question.
Conclusions: Sized patients were more satisfied than controls and fewer were interested in having a different size implant postoperatively. Sized patients indicated that preoperative sizing was both helpful and reasonably accurate in predicting final breast size. (Plast. Reconstr. Surg. 125: 1781, 2010.)
Patients pursuing breast augmentation have many options to consider before surgery, including surgeon, incision location, pocket plane, and multiple implant factors such as filler type, shape, profile type, texture, volume, and sometimes manufacturer. Implant diameter is another important variable, although it is less obvious to the layperson. Some have additional factors to consider such as the need for a simultaneous mastopexy that can be performed by several different methods and may be unilateral, bilateral, or require a different approach on each side. Ancillary procedures such as correction of inverted nipples or nipple reduction in the postpartum patient are options that add to the decision-making process.
Most patients today conduct considerable research, much of it Internet based, and usually see several physicians before committing to a definitive surgical plan. Arguably the most elusive factor to settle with certainty before surgery is implant size. Many patients have fixed notions of size based either on cup size, celebrity or Internet photographs, the experience of friends (both good and bad), or their personality. However, none of these factors is of proven benefit in selecting the proper implant size.
Verbal communication alone between the patient and physician, even if supplemented with adjunctive information as described above, is an unreliable method for determining implant size. When the decision is perceived to be a unilateral one on the part of the physician, the patient does not feel compelled to accept responsibility for that decision if she is disappointed after surgery. The need for additional surgery for a size change is associated with anxiety, urgency, and the belief that the surgeon is at fault or at least should bear the responsibility for the cost of replacement surgery.
Some surgeons tend to use a size larger than may be necessary to hedge their bets and avoid this situation, often perpetuating the folklore that patients always wish they were a little larger anyway.
Some surgeons tend to use a size larger than may be necessary to hedge their bets and avoid this situation, often perpetuating the folklore that patients always wish they were a little larger anyway.
Some practitioners have attempted to use a combination of chest wall measurements and “bust circumference” to determine implant size, whereas others have constructed tables that correlate implant volume with bra size for reference.1,2 Others rely on a set of specific tissue characteristics and measurements to determine optimal implant size.3–6 Although this latter method seeks to make size selection more scientific, it ultimately presents optimal size to the patient as a fait accompli without participation beyond her anatomy. This does not guarantee a happier patient, although it may provide the surgeon with stronger footing for discouraging pursuit of size change surgery later.
Many experienced surgeons seek to have the patient more actively involved in size selection in a way that will help preview the result. Some have described using rice or saline in a bag to estimate the size of the implant required.7–9 Today, there are Web sites on the Internet that describe the “rice test” for prospective patients to perform at home.10,11 A method of preoperative sizing that the authors have been using for the past several years and that constitutes the basis for this report consists of fitting patients with their desired bra size and placing various size sample silicone gel implants in the bra to simulate the result that each size would achieve (Fig. 1). This allows the patient to preview final breast size and, by participating in the sizing process, accept responsibility for the outcome together with the surgeon. The goal is to minimize the prospect for patient dissatisfaction after surgery that can ultimately lead to secondary surgery to change implant size.
 Fig. 1. Breast implant sizer box containing sample implant sizes. |
Patients and Methods
Technique of Preoperative Sizing
Preoperative sizing is performed at least two times before surgery. The first session is generally more time consuming and is usually done with the nursing staff, whereas the second session is done with the surgeon, as it is either largely confirmatory or the surgeon can give additional input to guide the process. Patients unable to clearly state a narrow range of preferred sizes are brought back for a third visit if necessary. The goal is to narrow the choice down to two sizes differing by not more than 25 cc. Patients are advised that this narrow range represents approximately one-eighth of a cup size and the final selection thereafter is best left as an intraoperative decision.
The process begins by fitting the patient with a larger bra that has underwires but minimal padding. This is most often a C cup, although a D cup may be used in some young nulliparous patients and a B cup in some older and more conservative postpartum patients. The chest circumference is variable and generally the same as the patient normally wears (even though many patients do not necessarily wear the correct size bra for their chest circumference).12 Patients are advised that the bra cup material adds volume by itself and that this varies depending on the type of bra. In our sizing bra, the extra volume measured 30 cc per side (Fig. 2). This volume can be added to the final size implant preferred by the patient during
the sizing process if she seeks the outside volume that includes the bra.
the sizing process if she seeks the outside volume that includes the bra.
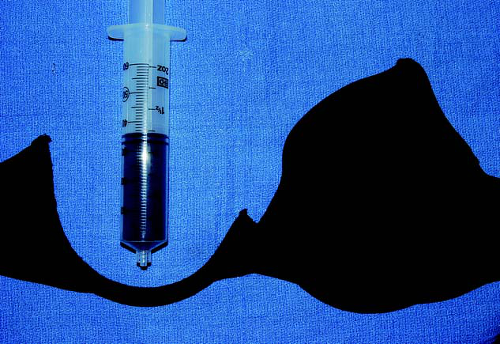 Fig. 2. A sample 34C bra is shown. The cup from one side has been cut off, rolled, and compressed within a syringe to demonstrate a volume of approximately 30 cc. The excised cup material weighed only 12 g.
Related posts: Breast Augmentation Breast Augmentation
 Breast Augmentation Breast Augmentation
 The Process of Breast Augmentation: Four Sequential Steps for Optimizing Outcomes for Patients The Process of Breast Augmentation: Four Sequential Steps for Optimizing Outcomes for Patients
 Acellular Dermal Matrices in Breast Augmentation Acellular Dermal Matrices in Breast Augmentation
 Brava and Autologous Fat Transfer Is a Safe and Effective Breast Augmentation Alternative: Results of a 6-Year, 81-Patient, Prospective Multicenter Study Brava and Autologous Fat Transfer Is a Safe and Effective Breast Augmentation Alternative: Results of a 6-Year, 81-Patient, Prospective Multicenter Study
 Understanding the Fascial Supporting Network of the Breast: Key Ligamentous Structures in Breast Augmentation and a Proposed System of Nomenclature Understanding the Fascial Supporting Network of the Breast: Key Ligamentous Structures in Breast Augmentation and a Proposed System of Nomenclature
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|