Breast Augmentation
David A. Hidalgo, M.D.
Jason A. Spector, M.D.
New York, N.Y.
From the Division of Plastic Surgery, Weill Cornell Medical College.
Received for publication April 9, 2012; accepted September 21, 2012.
Copyright © 2014 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0000000000000033
Disclosure: Neither author has a financial interest in any of the products or devices mentioned in this article. This work was not supported by outside funding.
Related Video content is available for this article. The videos can be found under the “Related Videos” section of the full-text article, or, for Ovid users, using the URL citations published in the article.
Learning Objectives: After studying this article, the participant should be able to: 1. Assess patient physical characteristics that influence implant selection. 2. Adopt a system to aid in implant size selection. 3. Become cognizant of the advantages and disadvantages of incision, pocket plane, and implant options. 4. Understand implant positioning concepts and aseptic implant handling methods. 5. Manage untoward postoperative sequelae 6. Understand secondary surgery concepts.
Summary: Breast augmentation is the most commonly performed aesthetic surgical procedure. Choices of incisions, pocket plane, and myriad implant characteristics constitute the basis for surgical planning. Analysis of physical characteristics and inclusion of the patient in implant selection contribute to overall satisfaction and reduce requests for secondary surgery. Technical expertise in implant positioning and aseptic handling helps to prevent capsular contracture, implant malposition, and other shape problems. Despite the need for secondary surgery in some, patient satisfaction is high. (Plast. Reconstr. Surg. 133: 567e, 2014.)
Breast augmentation is the most common aesthetic surgical procedure, with more than 300,000 performed in 2011.1 Choices of incisions, pocket plane, and implant characteristics, including shape, texture, filler, and volume, constitute the key decisions in surgical planning. Thoughtful analysis of physical characteristics and patient participation in the process are the most important factors in size selection. Knowledge of implant positioning and aseptic handling concepts contributes to successful outcomes and minimizes the need for secondary surgery. Patient satisfaction is high with this procedure, despite significant reoperation rates to treat capsular contracture, implant deflation, malposition, and other problems (References 2 and 3: Level of Evidence: Therapeutic, IV).2,3
Essentials of Preoperative Assessment and Management
Patient Evaluation
Each patient’s psychology, aesthetic sense, and anatomy must be critically assessed. Emotional stability is a mandatory prerequisite.4 Style of dress, makeup, tattoos, piercings, previous aesthetic procedures, community, and occupation reflect personality and aesthetics. Anatomic limitations must be explained to the patient.
Height and weight influence implant selection. For example, tall patients require larger volumes than short patients to achieve a similarly proportioned result. Thin patients are not well suited to saline implants. Idiosyncrasies in body morphology also play a role: patients with wide hips or shoulders look better with larger implants compared with those who are narrower.5
Chest wall shape is important to note.6 Pectus excavatum occurs occasionally, whereas pectus carinatum and Poland’s syndrome are rare.7 Central deformities are typically ameliorated sufficiently by breast augmentation alone. Deep pectus excavatum deformities can be treated simultaneously with a custom solid silicone implant made from a plaster moulage, but most patients decline this option. Poland’s syndrome, when severe, may
require adjunctive procedures, such as tissue expansion, fat grafting, and latissimus muscle transfer.7,8 A round thorax shape makes the breast axes diverge, causing the breasts to appear farther apart following augmentation. A rectangular thorax makes the axes parallel, so that the breasts appear closer together postoperatively.9 Hemithorax asymmetry due to differences in shape or relative protrusion can create an uneven breast foundation, suggesting different size implants despite equivalent breast volumes (Fig. 1).10 Scoliosis can cause vertical breast asymmetry requiring thoughtful implant positioning to minimize it.11
require adjunctive procedures, such as tissue expansion, fat grafting, and latissimus muscle transfer.7,8 A round thorax shape makes the breast axes diverge, causing the breasts to appear farther apart following augmentation. A rectangular thorax makes the axes parallel, so that the breasts appear closer together postoperatively.9 Hemithorax asymmetry due to differences in shape or relative protrusion can create an uneven breast foundation, suggesting different size implants despite equivalent breast volumes (Fig. 1).10 Scoliosis can cause vertical breast asymmetry requiring thoughtful implant positioning to minimize it.11
Existing breast volume influences implant filler choice. Small volume is not very compatible with saline implants, but as volume increases, there is less difference between saline and silicone.
Breast shape may limit implant selection. Vertically short breasts are prone to lower pole deformities as implant diameter increases. Similarly, breasts with constricted base diameters, such as tubular breast deformity, are challenging to aggressively augment and may require a more complex treatment strategy.12–14
Inframammary crease anatomy is also important. Minimal crease definition imposes little restriction on implant diameter selection, and therefore size. Glandular ptosis with a sharply defined crease located close to the areola represents the opposite extreme. This type is prone to double-bubble deformities as implant diameter increases.15
Tissue characteristics and skin quality are equally important factors. Postpartum patients with atrophic tissue and poor skin elasticity make visual and tactile implant concealment challenging, and also pose a risk of late lower pole descent. Conservatively sized silicone implants are the best choice in these patients. A concomitant mastopexy allows excision of some of the inelastic lower pole skin and enables placement of a smaller, lighter implant in more extreme cases.
Nipple hypertrophy and ptosis, common in postpartum patients, may be improved by circumferential skin excision at the nipple base. (See Video, Supplemental Digital Content 1, which demonstrates a nipple reduction. This video is available in the “Related Videos” section of the full-text article on PRSJournal.com or, for Ovid users, at http://links.lww.com.easyaccess2.lib.cuhk.edu.hk/PRS/A952.) Reduction in both height and diameter can be achieved by the top-hat reduction method.16 Treating this condition is simple and enhances the overall result.
Nipple-areolar position asymmetry is magnified by breast augmentation (Fig. 2). A unilateral circumareolar mastopexy or a Y-scar mastopexy can be considered depending on the severity of the problem.17
The larger the areolar diameter, the more it tends to stretch following surgery. Conservative circumareolar
excision should be considered with diameters approaching 6 cm. Circumareolar excision must be coupled with a periareolar purse-string suture, typically with nonabsorbable suture material, in order to provide a lasting result.
excision should be considered with diameters approaching 6 cm. Circumareolar excision must be coupled with a periareolar purse-string suture, typically with nonabsorbable suture material, in order to provide a lasting result.
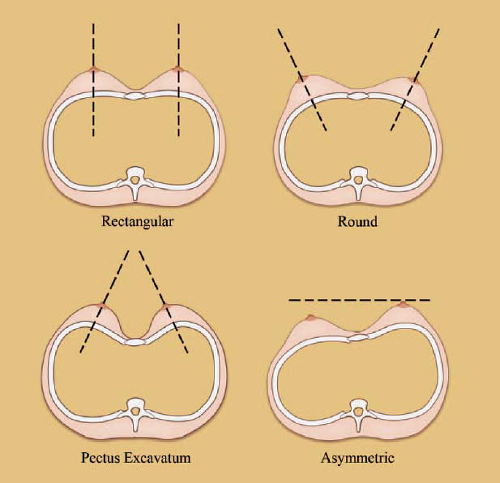 Fig. 1. Chest wall shape can affect the axes of the breasts and their relative projection. |
 Video 1. Supplemental Digital Content 1, which demonstrates nipple reduction, is available in the “Related Videos” section of the fulltext article on PRSJournal.com or, for Ovid users, at http://links.lww.com.easyaccess2.lib.cuhk.edu.hk/PRS/A952. |
Implant Selection
Size (volume and diameter) is arguably the most critical aspect of implant selection, followed by filler type. Second-tier factors include shape, profile, and surface texture.
The differences between textured and smooth implants have been debated (Reference 19: Level of Evidence: Therapeutic, I).18,19 Current evidence holds that smooth implants are more prone to capsular contracture in the subglandular plane.20 A difference between the two types has not been proven in the subpectoral plane.19 Smooth implants are currently used in approximately 90 percent of patients in the United States.21
Round implants are used in 95 percent of patients in the United States today.21 Superior aesthetic results
using anatomic implants remain unproven. Implant rotation requiring additional surgery can occur with these devices (Reference 23: Level of Evidence: Therapeutic, IV).22,23 Unlike in breast reconstruction, a different scenario, there is no clear role for anatomic implants in breast augmentation.
using anatomic implants remain unproven. Implant rotation requiring additional surgery can occur with these devices (Reference 23: Level of Evidence: Therapeutic, IV).22,23 Unlike in breast reconstruction, a different scenario, there is no clear role for anatomic implants in breast augmentation.
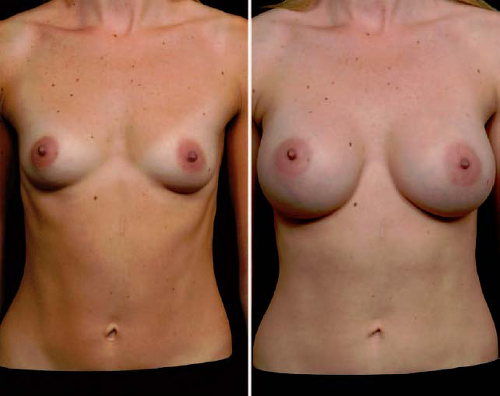 Fig. 2. (Left) Preoperative nipple-areolar position asymmetry. (Right) The asymmetry is magnified following augmentation, but within acceptable limits. |
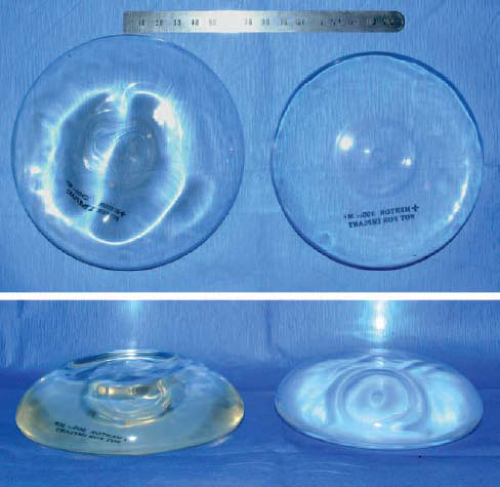 Fig. 3. A 300-cc standard profile implant is shown on the left. The 300-cc implant on the right has a higher profile but a smaller diameter in comparison. It also appears to be filled tighter and does not exhibit the wrinkling evident in the standard profile implant. The latter feature is an indication for its use in thin patients. |
Implant profile is a variable that aids in achieving maximum volume in patients having narrow chests, breast base diameters, or both. Higher profile implants have smaller diameters that allow placing maximum volume in these cases. Patients with wide chests or breast base diameters do best with regular profile implants (Fig. 3 and Table 1).
Table 1. Implant Profile Selection | ||||||
|---|---|---|---|---|---|---|
| ||||||
Selection of saline versus silicone filler is influenced by anatomy, as previously described. Advantages of saline implants include smaller incisions with possible remote locations, no special long-term monitoring, and results that may endure for decades. Silicone implants have less wrinkling and palpability, and no risk of deflation. Approximately 60 percent of implants used in the United States today are gel filled.21
Size is usually the most important implant variable to the patient. Magazine photographs, cup sizes, and friends’ experiences are not reliable measures for determining size. One recommended method computes optimal size based on breast base width, anterior skin stretch, upper pole pinch thickness, inframammary fold pinch thickness, and stretched nipple-to-fold distance.24–26 This analytic method determines optimal implant dimensions based on individual anatomic characteristics.
Preoperative sizing is another method that is more subjective in its approach. It consists of placing sample implants in a bra to preview a range of possible results.27 The surgeon first determines a size range suggested by height, weight, and body habitus that is also mindful of breast anatomy restrictions. This process shares ownership of the final decision between the patient and the surgeon. It has been shown to minimize requests for size-change surgery.27
Patient Education
Comprehensive patient education should include implant options, associated risks, anatomical restrictions, and potential problems that can lead to secondary surgery. Given that implants are prosthetic medical devices, providing informed consent requires imparting considerable information. Providing a written document in which the patient initials each paragraph is one effective way to disclose all possibilities and ensure that the information has been received (see Appendix).
Besides size, implant filler type is a key decision for the patient. When informed that the notion that silicone
implants “look” more natural than saline is mistaken, the patient can base her choice between the two types on other reasons (Table 2).
implants “look” more natural than saline is mistaken, the patient can base her choice between the two types on other reasons (Table 2).
Table 2. Patient Education: Saline versus Silicone Implants | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
Breast implants have a rare association with anaplastic large cell lymphoma.28–30 Current evidence indicates that the risk of developing anaplastic large cell lymphoma is 0.1 to 0.3 per 100,000. It usually presents as a seroma after 1 year.31 Anaplastic large cell lymphoma is typically indolent, and treatment by implant removal and capsulectomy is effective. Adjuvant therapy with radiation or chemotherapy is not routinely recommended.32,33 Approximately 34 cases have been reported in the medical literature to date. This notable new development should be included in the patient education process.
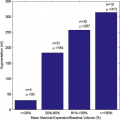
Breast augmentation by fat grafting following external tissue expansion is a recent alternative to using implants.34 The developers claim safety of large-volume fat injections and acknowledge that final volume is more modest compared with implants, that there is benefit from simultaneous liposuction, and that the procedure can be performed in a few hours.35,36 This method is still under development and evaluation for long-term safety and efficacy.
Advantages and Disadvantages of Treatment Options
Incisions
Axillary
Axillary incisions for saline implant placement are advantageous because they avoid breast scars (Table 3). Young patients with good shape and substantial volume are ideal candidates (Fig. 4). Either blunt or endoscope-assisted dissection can be used.37 Blunt dissection is simpler but requires experience and finesse. Surprisingly, hematomas are rare. (See Video, Supplemental Digital Content 2, which demonstrates transaxillary subpectoral augmentation without endoscopy. This video is available in the “Related Videos” section of the full-text article on PRSJournal.com or, for Ovid users, at http://links.lww.com.easyaccess2.lib.cuhk.edu.hk/PRS/A953.) Endoscopic technique is more complex and has a normal hematoma risk because sharp dissection is employed. Superior implant malposition is more likely using axillary incisions due to the remote approach to inframamary crease position management.38 Silicone implant placement through this incision is not widely practiced but can be done.39 Axillary incisions do not interfere with sentinel lymph node biopsy.40,41 Revisional surgery usually requires a second incision. This route can be more painful.
Table 3. Incision Options and Indications | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Periareolar
Periareolar incisions, given their central location, provide arguably the best exposure of the implant pocket. They facilitate controlled inframammary crease lowering under direct vision (Fig. 5).5 This exposure is particularly advantageous in secondary cases when capsulectomy or capsulorrhaphy is necessary. There is evidence, however, that periareolar breast tissue is less sterile and that the incidence of capsular contracture is higher.42,43
Periareolar incisions are typically inconspicuous provided they are placed precisely at the junction of the color change. There is little tension, so scar quality tends to be excellent and hypertrophy rare.
A small areolar diameter may preclude its use for silicone implant placement. Periareolar incisions can also be problematic in postpartum women with thin, atrophic tissues. The forces of wound contraction may cause a depressed scar. This may require secondary correction using acellular dermal matrix to restore shape (Fig. 6).44
Inframammary
Inframammary incisions remain the most popular choice today.45 They afford immediate access to the subpectoral plane without disturbing the gland. This approach is typically less painful and affords the longest incision possible, an advantage with stiff “form-stable” textured silicone implants. It is preferred for postpartum patients with thin atrophic breast tissue (Fig. 7 and Table 3).
Related posts:
 Breast Augmentation
Breast Augmentation
 The Process of Breast Augmentation: Four Sequential Steps for Optimizing Outcomes for Patients
The Process of Breast Augmentation: Four Sequential Steps for Optimizing Outcomes for Patients
 Preoperative Sizing in Breast Augmentation
Preoperative Sizing in Breast Augmentation
 Acellular Dermal Matrices in Breast Augmentation
Acellular Dermal Matrices in Breast Augmentation
 Brava and Autologous Fat Transfer Is a Safe and Effective Breast Augmentation Alternative: Results of a 6-Year, 81-Patient, Prospective Multicenter Study
Brava and Autologous Fat Transfer Is a Safe and Effective Breast Augmentation Alternative: Results of a 6-Year, 81-Patient, Prospective Multicenter Study
 Understanding the Fascial Supporting Network of the Breast: Key Ligamentous Structures in Breast Augmentation and a Proposed System of Nomenclature
Understanding the Fascial Supporting Network of the Breast: Key Ligamentous Structures in Breast Augmentation and a Proposed System of Nomenclature
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


