Key points
• Look at the patient: Your eye is the best tool to evaluate both the premorbid injury as well as your repair. It is imperative that you learn how to really “see” the anatomy and appreciate the subtle characteristics of each patient’s facial form. Always evaluate preinjury pictures of your patient because they can both guide your restoration.
• Consider form and function: Recognize that there is more to repair than anatomy. The surgeon has not completed the restoration until every element, including expression and emotion, has been considered.
• There may be posttraumatic premature aging of the face due to localized loss of fat and potential descent of the facial soft tissue, and the patient may benefit from subsequent application of the aesthetic techniques of fat grafting tissue and/or resuspension.
• Beauty may be skin deep but ugly goes to bone: No soft tissue reconstruction can be successful without first having bone and occlusion in the proper alignment. Skeletal deficiencies or asymmetries will require correction in conjunction with soft tissue techniques to achieve an optimal result.
• Treat every trauma patient as you would a cosmetic patient: The reconstructive surgeon attempts to reconstruct the damaged to the “normal.” The aesthetic surgeon attempts to elevate the “normal” to the beautiful. There is no reason why both cannot be done in the posttraumatic patient.
• Prepare for the long haul: One hopes to accomplish the basic reconstruction during the first operation, but the process of healing and subsequent corrections may extend over years. Preparing the patient and the family for an extended reconstruction is best done at the time of the initial surgery.
Introduction
The reconstruction of posttraumatic of facial deformities by maxillofacial surgeons was launched at the time of the Great War (World War I) to treat soldiers who had sustained severe facial injuries in trench warfare and thus severe facial disfigurement. Treatments since then have evolved from tubed pedicle flaps and plaster dressings to advanced techniques, such as microsurgical reconstruction, rigid fixation, custom-fabricated implants, autologous fat transfer, and even face transplantation. The advances in the approach to posttraumatic facial reconstruction have given the surgeon many tools to restore a patient’s facial form after an injury. For the purpose of this chapter, posttraumatic injuries will be grouped into occlusal and nonocclusal posttraumatic deformities.
Patient evaluation
Patients may exhibit posttraumatic deformities in spite of excellent primary reconstruction. In fact, it is common for a patient who undergoes major surgery after facial trauma to have no desire for further surgery. However, as time passes and residual deformities become apparent, the patient changes his or her mind and desires additional procedures to optimize return to the “normal” preoperative facial form. This cycle can continue until either the patient obtains an acceptable appearance or the surgeon feels that additional procedures are not justified.
History
A thorough history is critical in the evaluation of this population. It is important to have details about the initial nature of the injury and the types and number of previous surgeries that were performed. If microvascular surgery is to be undertaken, it is important that the surgeon be aware of previous operations to determine what options are available for anastomosis in the region of interest. Because the success of many types of surgical procedures depends on the health of the patient, it is important to obtain an accurate medical history to ensure that there are no clotting disorders, anatomic abnormalities, history of radiation, or other patient factors that may increase the morbidity of the operation.
Differential diagnosis
Because the patient reports the nature of the problem as posttraumatic, a true differential diagnosis may not be possible. In lieu of a differential diagnosis, there is a wide variety of approaches for any given problem. Based on the patient’s medical condition, problem, and enthusiasm to undergo a procedure, the surgeon and the patient together can develop a treatment plan that will maximize the chances of returning the patient’s face to its normal form while minimizing perioperative morbidity.
Physical examination
The physical examination should be approached in two aspects: (1) the individual tissue levels from the skeleton toward the cutaneous surface and (2) the anatomic regions of the face and cranium.
Tissue analysis
An excellent method to assess the skeletal tissue is three-dimensional (3D) computed tomography (CT). This, combined with clinical examination, gives the surgeon an excellent view of the degree, position, and quality of skeletal bone. The symmetry in size and position of paired structures can also be assessed.
The skeletal structures are best visualized on the CT scan and are evaluated for volume, position, and symmetry. Deficient skeletal tissue can be augmented with bone grafts, alloplastic materials, or free tissue transfer. Skeletal structures that are malpositioned or asymmetrical can be repositioned with osteotomies. Some asymmetries can be camouflaged by using bone grafts or alloplastic implants if an osteotomy is unfeasible.
The soft tissue deep to the skin can be evaluated on the CT scan, but the physical examination frequently yields more information. The presence of scarring, radiation damage, or tissue deficiency informs the surgeon as to the quality and quantity of soft tissue and dictates the need for replacement. Soft tissue not only contributes to aesthetic quality but also to functional quality. In areas of severe scarring, reconstruction may need to be undertaken to return normal range of motion and function. This is particularly true in the patient who sustained third-degree burns.
The skin and subcutaneous tissue are assessed for volume, pliability, and appearance. Subcutaneous soft tissue deficiencies between the dermis and the underlying musculature can frequently be treated with fat grafting. However, thick scarring on aesthetic skin may require excision and replacement through various treatment options. Finally, large areas of tissue deficiency in both volume and skin quality may require microvascular tissue transfer.
Anatomic analysis
Calvarium: An evaluation of the calvarium is done to ensure that there is protective coverage of the underlying brain and a normal contour. Soft tissue is independently evaluated to make sure that there is adequate vascularized soft tissue coverage over the underlying calvarium.
Orbits/Canthi: The orbits should be evaluated for position, size, and symmetry. The globe is examined for the presence of enophthalmos and restricted ocular movement. Additionally, the medial canthi should be evaluated to see if there is any history of canthal dehiscence, which would be suspected in the presence of telecanthus. The presence of upper lid ptosis may result from injury and should also be assessed.
Nose: The nose is the central structure to the face, and any abnormality in its symmetry or form likely will result in patient concerns. The nose is evaluated for both form and function, as described in Chapters 28 and 29 .
Malar region: The malar region should demonstrate symmetry and adequate projection with no visible contour irregularity.
Maxilla: The maxilla is assessed for the presence of a midline deviation, occlusal cant, and malocclusion. Missing teeth and bone should also be noted and their rehabilitation incorporated into the final treatment plan.
Mandible: Intraorally, the mandible and the dentition are evaluated for midline discrepancies, occlusal discrepancies, and continuity defects. Externally, the mandible should be evaluated for symmetry, normal contour, and good soft tissue projection.
Chin: The chin is assessed as described in the genioplasty chapter. The surgeon should note any midline discrepancy, asymmetry, or insufficient vertical or sagittal projection.
Imaging and diagnostic materials
Fine-cut CT scans are essential for performing a detailed analysis of the underlying facial skeleton. They also reveal any radiopaque implants or fixation devices. The scans are useful in virtual surgical planning (VSP), where surgical plans are developed on imaging before going to the operating room. The scans are also important in designing custom implants, surgical cutting guides, and surgical splints.
When the occlusion is involved in the deformity, it is important to have a set of dental casts to articulate the occlusion and identify any occlusal discrepancies. If discrepancies are noted and the patient desires to have the correction incorporated into the treatment plan, VSP can be performed by using 3D CT. ,
Indications and contraindications
This chapter summarizes the myriad of techniques and their contraindications and indications described in other chapters in this textbook.
Preoperative planning
The approach to facial reconstruction depends on whether the original injuries involved the occlusion. Because occlusal injuries require a unique approach, they will be addressed in a separate section within this chapter.
Nonocclusal posttraumatic reconstruction
The evaluation of the patient who presents for posttraumatic reconstruction without an occlusal injury is based primarily on photographs and CT scans.
Accurate photographic documentation of the patient is important in developing the treatment plan. Images of the patient before treatment are invaluable in helping the surgeon identify the patient’s preinjury facial form. Additionally, 3D CT scans are necessary for identifying any skeletal deformity and developing the treatment plan. The broad adoption of VSP has led to its acceptance as an extremely useful tool in the diagnosis, treatment planning, and implant fabrication for skeletal deformities. The individual techniques used in posttraumatic reconstruction are described elsewhere in this text. The following case descriptions will serve to show the patient evaluation and treatment approach using these tools.
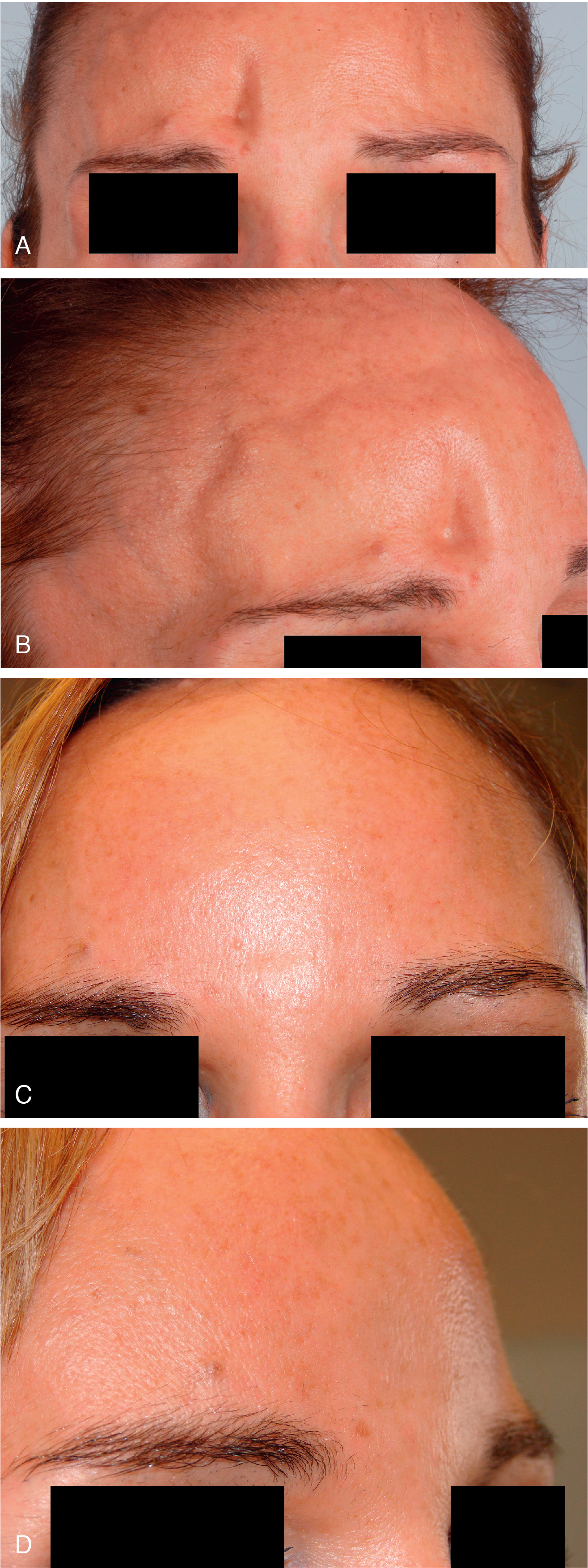
Case 1: Cranial deformity ( fig. 42.1 )
This female patient ( Fig. 42.1 A, B) sustained an injury to her right frontal bone and superior orbit. She presented with a desire to restore her preinjury appearance. A CT scan revealed an abnormal cranial contour, as well as thin soft tissue overlying the deformity. Hydroxyapatite bone cement was used to restore the skeletal contour, and structural fat grafts were injected to increase the fullness of the atrophic overlying soft tissue (see Fig. 42.1 C, D).